Abstract
This systematic review aimed to understand the role of physical activity in reducing social isolation and loneliness among older adults, while also analysing its effects on physical, psychological and social wellbeing during the ageing process. The literature search was conducted in the PubMed database, following the PRISMA guidelines and the PICOS framework. Studies involving adults aged 60 years or over were considered, provided that they included interventions based on physical activity, exercise, walking, tele-exercise, yoga or multicomponent programmes. After an initial identification of 981 articles, 7 studies were selected for qualitative analysis. The findings suggest that regular physical activity may contribute to reducing loneliness and social isolation, particularly when performed in groups, in community settings, or when combined with socialisation, social support and regular supervision. In addition, the studies analysed reported benefits in quality of life, mood, functional autonomy, mobility and psychological wellbeing. Digital interventions and tele-exercise were also shown to be useful alternatives, especially for older adults with mobility limitations or those living in rural areas, although their impact on loneliness appears to depend on the presence of meaningful social interaction. It is concluded that physical activity represents an important strategy for promoting more active, healthy and socially integrated ageing.
Highlights
- Physical activity may contribute to reducing loneliness and social isolation among older adults.
- Group- and community-based exercise programmes provide greater social and psychological benefits than exercise performed alone.
- Physical activity improves mobility, functional autonomy, mood and overall quality of life in older adults.
- Tele-exercise and digital interventions are useful alternatives, particularly for older adults with mobility limitations or living in rural areas.
- Physical activity combined with social interaction and support appears more effective in reducing loneliness than exercise alone.
1. Introduction
With the increase in life expectancy, there has also been significant growth in the older population, which requires greater attention to public policies and health promotion strategies [1]. In this context, physical activity emerges as an essential tool for the prevention and maintenance of health, contributing to active and healthy ageing [6].
Ageing is a process associated with several morphological [2], physiological [3], biochemical [5] and psychological [4] changes that occur in the human body and lead to the gradual loss of an individual’s adaptive capacity [5]. The pursuit of a better quality of life has been one of the determining factors for successful ageing, and regular physical activity has contributed to the prevention and control of diseases, as well as to health promotion [8]. Although the benefits of physical activity are widely known, a large proportion of the older population still does not engage in it due to numerous internal and external barriers, as well as other barriers created by the individuals themselves, which reduce their engagement in healthy practices [7].
This study aims to understand the role of physical activity in reducing social isolation in ageing, and how physical activity influences morphological, physiological, biochemical, and psychological changes.
Social isolation and loneliness are currently two of the main psychosocial challenges associated with ageing, being recognised as relevant social determinants of health and well-being in older adults [9], [10].
As age advances, several factors may increase vulnerability to social isolation and loneliness, namely retirement, the loss of family members or friends, widowhood, reduced mobility, chronic diseases, sensory limitations, and reduced participation in social activities [9], [10]. These factors may contribute to a decrease in opportunities for social interaction and to a greater perception of distance from the community, making loneliness a relevant phenomenon not only from an emotional perspective, but also from a functional and clinical point of view [9], [11].
Physical activity has been widely recognised as an essential strategy for promoting healthy ageing, not only because of its physiological and functional benefits, but also because of its potential impact on the psychological and social dimensions of well-being [9], [11]. In older adults, regular physical activity may support the maintenance of autonomy, mobility, self-esteem, and social participation, factors that may contribute to reducing social isolation and loneliness [11], [12].
The relationship between physical activity and social isolation may be explained through different mechanisms. Firstly, exercise programmes, especially when carried out in groups, create opportunities for interpersonal contact, the sharing of experiences, and the development of social support networks [11], [12]. Secondly, improvements in functional capacity may make it easier to leave the house, participate in community activities, and maintain meaningful social roles, reducing dependence and increasing the perception of control over daily life [11]. In addition to direct social effects, physical activity may influence loneliness through psychological benefits, such as improved mood, reduced depressive symptoms, increased self-efficacy, and the promotion of a greater sense of belonging [11], [13]. However, the literature suggests that physical activity alone may not be sufficient to reduce loneliness, being more effective when combined with components of social interaction, community support, health education, or regular follow-up [11], [12].
This study aims to understand the role of physical activity in reducing social isolation during the ageing process, analysing how regular physical exercise can contribute to better social integration, the promotion of well-being, and improved quality of life among the older population. It also seeks to understand how physical activity influences changes associated with ageing, namely at the morphological, physiological, biochemical, and psychological levels, considering its possible effects on maintaining autonomy, preventing functional decline, and promoting more active and healthy ageing.
In addition, the study seeks to analyse whether participation in physical activity programmes, especially in group contexts, can promote social contact, reduce feelings of loneliness, and increase motivation, self-esteem, and the perception of social support among older adults. Regular physical activity contributes to reducing social isolation in ageing by promoting improvements in quality of life, functional autonomy, psychological well-being, and social relationships among older adults, while also helping to attenuate some of the morphological, physiological, and biochemical changes associated with the ageing process.
2. Methods
2.1. Search strategy
This systematic review was conducted in accordance with the PRISMA guidelines (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) and structured based on the PICOS model: Population, Intervention, Comparison, Outcomes, and Study Design.
The bibliographic search was carried out in the PubMed database with the aim of identifying scientific studies that analysed the relationship between physical activity, ageing, and social isolation in older adults.
Table 1PICOS structure used to define the eligibility criteria
Element | Description |
Population (P) | Older adults aged 60 years or over |
Intervention (I) | Physical activity programmes, physical exercise, walking, group exercise, tele-exercise, yoga, or other movement-based interventions |
Comparison (C) | Physical activity programmes, physical exercise, walking, group exercise, tele-exercise, yoga, or other movement-based interventions |
Outcomes (O) | Social isolation, loneliness, psychosocial well-being, mental health, quality of life, and social participation |
Study design (s) | Experimental studies, quasi-experimental studies, randomised controlled trials, pilot studies, and intervention studies |
The search expression used was the following: (“group exercise” OR “exercise program” OR “physical activity”) AND (“older adults” OR elderly OR aging) AND (“social isolation” OR loneliness). | |
2.2. Inclusion and exclusion criteria
The articles were selected based on the inclusion and exclusion criteria defined in Table 2, ensuring the coherence and methodological relevance of the studies considered [16].
Table 2Inclusion and exclusion criteria of the studies
Inclusion criteria | Exclusion criteria |
Studies conducted with older adults | Population under 60 years of age |
Studies that included physical activity, physical exercise, or movement-based programmes | No intervention related to physical activity |
Studies that assessed outcomes related to social isolation, loneliness, well-being, or mental health | Assessment of components other than loneliness, social isolation, or psychosocial well-being |
Intervention studies, randomised controlled trials, pilot studies, or quasi-experimental studies from the last 10 years | Reviews, editorials, comments, theses, conference abstracts, or opinion articles |
Studies with full text available | No accessible full text |
2.3. Study selection process
The selection of studies took place in two phases:
– Reading of titles and abstracts, with the aim of excluding articles that did not fit the topic of the review.
– Full-text reading of potentially eligible articles, applying the previously defined inclusion and exclusion criteria.
After removing duplicate studies and excluding articles that did not meet the established criteria, the studies that analysed the relationship between physical activity, ageing, social isolation, and loneliness in older adults were selected. These studies were considered for qualitative analysis. The complete selection process is represented in the PRISMA flow diagram in Fig. 1.
2.4. Data Coding and Extraction
Data extraction and coding were carried out using a structured grid in order to ensure a clear, uniform, and transparent organisation of the information collected [15].
Information was extracted regarding the author and year of publication, type of study, sample characteristics, participants age, type of intervention, programme duration, application context, variables assessed, main results, and conclusions of the included studies.
2.5. Assessment of methodological quality
The methodological quality of the included studies was analysed by considering the clarity of the objectives, the methodological design, the description of the sample, the existence of a comparison group, the instruments used, and the presentation of the results.
Greater relevance was attributed to studies with an experimental design, especially randomised controlled trials, as they present greater methodological robustness. Studies that used validated instruments to assess loneliness, social isolation, mental health, and quality of life were also valued.
Fig. 1Flowchart (Prisma)
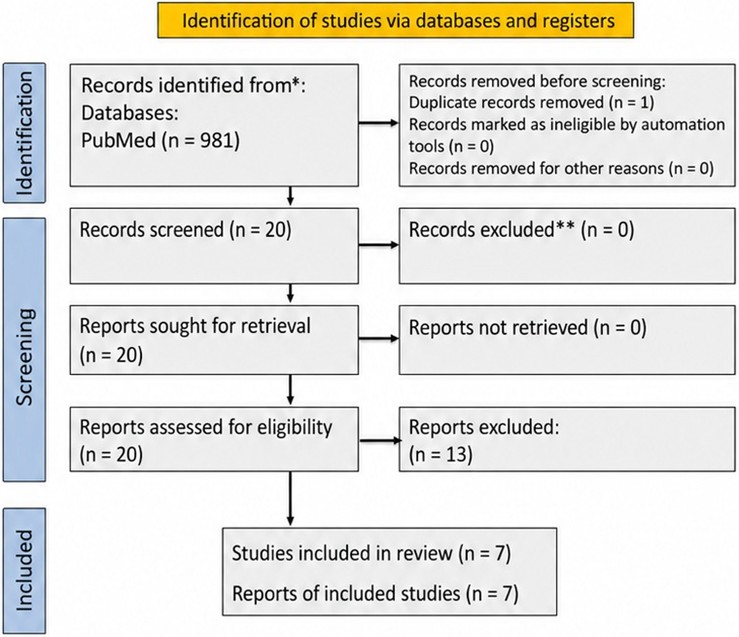
Table 3Variables included in data coding and extraction
Extracted variables | Information collected |
Author and year | Identification of the study |
Type of study | RCT, pilot study, quasi-experimental study, or other |
Sample | Number of participants included |
Age | Age range of the participants |
Intervention | Type of physical activity or exercise applied |
Duration | Total intervention period |
Context | Community, online, care home/institution, or other |
Outcomes assessed | Loneliness, social isolation, mental health, quality of life, and psychosocial well-being |
Main results | Effects observed after the intervention |
Conclusion | General interpretation of the study results |
3. Results
The selection of studies took place in two stages. Initially, the titles and abstracts were screened, followed by the full-text reading of texts considered potentially eligible. The process of identifying and selecting the studies followed the PRISMA format.
The initial search identified 981 articles. After applying the defined filters, 21 studies were retained for analysis. Subsequently, 1 duplicate article was removed, resulting in 20 articles for full-text reading. Of these, 13 studies were excluded because they did not meet the previously established inclusion criteria, resulting in a final sample of 7 studies included in the systematic review.
Table 4Summary of the included studies on physical activity interventions in older adults
Author (Year) | Study type | Sample | Age | Intervention | Duration | Context | Main variables | Main results | Conclusion |
Gust et al. [16] | RCT | 211 healthy older adults | Older adults | Aerobic exercise, low vs. moderate intensity | 16 weeks | Community | Depression, loneliness, emotional functioning | Reduction in depression; greater improvement in loneliness in the higher-intensity exercise group | Exercise may improve emotional and social dimensions in older adults. |
Nettlefold et al. [17] | Hybrid study, implementation + effectiveness | 1126 | ≥60 years | “Choose to Move” program, physical activity + social support | 3 months | Community | Physical activity, social isolation, loneliness | Increased physical activity and improvements in social isolation and loneliness | Community-based physical activity programs may reduce isolation and loneliness. |
Gen et al. [18] | RCT | 64 | ≥60 years | Multicomponent program, exercise + education + self-monitoring | 8 weeks | Community | Loneliness, physical activity | Significant reduction in loneliness; no relevant changes in physical activity | Multicomponent interventions may reduce loneliness even without a major increase in physical activity. |
Zengin et al. [19] | RCT | 30 | ≥65 years | Tele-exercise, supervised online exercise | ~12 weeks | Social isolation during COVID-19 | Quality of life, loneliness, mood | Improvements in mood and quality of life; loneliness did not worsen in the exercise group | Tele-exercise may help isolated older adults maintain well-being and mood. |
Jones et al. [20] | Pilot RCT | 35 | ≥65 years | Exercise + socialization + health education | 10 weeks | Community | Loneliness, physical function | Improved physical function and reduced loneliness | Exercise combined with socialization may benefit older adults at risk of isolation. |
Mastrogiovanni et al. [21] | RCT | 80 | ≥60 years | Digital intervention, physical activity + education + social support | 11 weeks | Online/community | Psychological distress, loneliness | Reduced psychological distress; no significant changes in loneliness | Digital interventions may improve mental health, but do not always reduce loneliness. |
Teo et al. [12] | RCT | 70 | ≥60 years | Telehealth yoga, group-based physical activity | 10 weeks | Rural/online | Loneliness, social isolation | Loneliness decreased in both groups, with no significant difference between groups | Online yoga was acceptable, but did not show a clear effect on loneliness or social isolation. |
Data extraction was carried out using a structured grid, including: study design, participant characteristics, sample age, type of intervention, programme duration, application context, comparison group, objectives, outcomes related to loneliness, social isolation, mental health, and quality of life, as well as the main results and conclusions of the included studies.
4. Discussion
This systematic review aimed to understand how physical activity can contribute to reducing social isolation and loneliness in older adults. The initial hypothesis was that regular physical activity contributes to reducing social isolation and loneliness in ageing. Overall, the results found allow this hypothesis to be partially confirmed, since not all studies demonstrated significant reductions in loneliness or social isolation. Even so, most studies point to physical, psychological, and social benefits associated with physical exercise in older adults.
Seven studies were included, involving different types of intervention, namely aerobic exercise, community-based physical activity programmes with social support, multicomponent interventions, tele-exercise, online yoga, and digital programmes. The samples ranged from 30 to 1126 participants, aged 60 years or over, and the duration of the interventions ranged from 8 to 16 weeks. Most studies took place in community settings, although online or hybrid interventions were also included, which are especially relevant for older adults with mobility difficulties, those living in rural areas, or those experiencing isolation.
The most recent studies reinforce the importance of programmes that combine physical activity with social support. [17], through the Choose to Move programme, found improvements in physical activity, mobility, social isolation, and loneliness in older adults, showing that community-based programmes can be effective when they are accessible and adapted to the needs of the older population. [18] also demonstrated that a multicomponent intervention focused on physical activity and reducing loneliness in socially frail older adults contributed to reducing loneliness, even without major changes in physical activity levels.
The results of this review indicate that physical activity may be an important strategy for reducing loneliness and promoting greater social integration among older adults. The effects appear to be more evident when exercise is performed in groups, in a community context, or combined with components of socialisation, health education, and regular follow-up. This suggests that the benefits of physical activity do not depend only on movement itself, but also on opportunities for social contact, the creation of routines, a sense of belonging, and increased social support.
In addition to social benefits, the included studies also demonstrated improvements at the psychological level. [16] found that supervised aerobic exercise over 16 weeks contributed to a reduction in depressive symptoms, and that the group exposed to moderate-intensity interval exercise showed greater improvement in loneliness compared with the lower-intensity group. These results show that physical activity can act simultaneously on emotional and social dimensions, contributing to healthier ageing.
Digital interventions and tele-exercise showed more varied results. [19] observed improvements in mood and quality of life through tele-exercise, while [21] found that yoga via telehealth was feasible and acceptable, but did not demonstrate a clear effect on reducing loneliness and social isolation. Similarly, [21] found that a multicomponent digital intervention reduced psychological distress, but did not produce significant changes in loneliness. Therefore, online interventions may be useful, but seem to require greater social interaction in order to have a more consistent impact on loneliness.
Despite the positive results, the included studies present some limitations. Firstly, there is great diversity among the interventions, both in terms of the type of exercise and the duration, intensity, frequency, and application context, which makes direct comparison between studies difficult. Secondly, some samples were small, as in the studies by [21] and [20], which limits the generalisation of the results. Thirdly, several interventions had a short duration, between 8 and 12 weeks, which does not allow us to understand whether the positive effects are maintained in the long term.
Another important limitation is related to the difference between loneliness and social isolation. Loneliness is a subjective experience, related to the individual perception of a lack of social connection, whereas social isolation is more objective and depends on the quantity and frequency of social contacts. Therefore, an intervention may improve social participation without significantly reducing loneliness, or it may improve psychological well-being without greatly changing the older adult’s social network. The World Health Organization itself recognises that loneliness and social isolation have an important impact on physical health, mental health, quality of life, and longevity, and are complex problems that require multidimensional responses [8].
Despite these limitations, the results of this review reinforce that physical activity should be valued as a relevant strategy to promote active and healthy ageing. Regular exercise can improve mobility, autonomy, mood, self-esteem, and quality of life, factors that facilitate social participation and reduce the risk of isolation. The WHO also highlights that regular physical activity provides physical and mental benefits, including the reduction of symptoms of depression and anxiety and the improvement of general well-being [22].
Future research should seek to understand which types of intervention are most effective in reducing loneliness and social isolation in older adults. It would be important to compare in-person, digital, and hybrid programmes, as well as to analyse the impact of exercise intensity, frequency, and duration. Studies with larger samples, greater participant diversity, and longer follow-up periods are also needed in order to understand whether the effects are maintained over time.
In addition, future studies should assess loneliness, social isolation, quality of life, mental health, and functionality separately, using validated instruments. It would also be relevant to investigate interventions that combine physical exercise, socialisation, health education, psychological support, and community follow-up. In this way, programmes aimed at the older population may become more complete and effective, not only in improving physical condition, but also in promoting psychological well-being and social integration.
5. Conclusions
This systematic review made it possible to understand that physical activity plays an important role in promoting the physical, psychological, and social well-being of older adults. The studies analysed suggest that physical exercise programmes, especially when carried out in groups, may contribute to reducing loneliness and social isolation.
Overall, regular physical activity promotes social participation, improves mood, and enhances quality of life. Digital interventions and tele-exercise also appear to be useful alternatives, especially for older adults in rural contexts or with mobility difficulties, although they seem to be more effective when they include social interaction and regular follow-up.
Thus, it is concluded that physical activity should be valued as a fundamental strategy for more active, healthy, and socially integrated ageing. Future studies should analyse which intervention formats are most effective in reducing loneliness and social isolation in this population.
\
References
-
J. N. da Silva Filho, “Physical exercise for health promotion in older adults: Review and experiment with participants from an extension project at the Rio de Janeiro State University,” (in Portuguese), Rio de Janeiro State University, Rio de Janeiro, Brazil, 2025.
-
S. Vaz, A. Félix, P. Pires, B. Magalhães, J. Seco-Calvo, and A. Novo, “The influence of physical activity on the respiratory capacity of individuals with ventilatory impairment,” (in Portuguese) in Physical Activity – a Central Concept in Rehabilitation Nursing, Coimbra, Portugal: Escola Superior de Enfermagem de Coimbra, 2025.
-
M. Mrejen, L. Nunes, and K. Giacomin, Population Aging and the Health of Older Adults: is Brazil Prepared. (in Portuguese), São Paulo, Brazil: Instituto de Estudos para Políticas de Saúde (IEPS), 2023.
-
Rodrigues and M. E. B., “Psychological and physical benefits of regular physical activity in older adults,” (in Portuguese), Polytechnic Institute of Guarda, Guarda, Portugal, 2014.
-
F. O. Asejeje and O. B. Ogunro, “Deciphering the mechanisms, biochemistry, physiology, and social habits in the process of aging,” Archives of Gerontology and Geriatrics Plus, Vol. 1, No. 1, p. 100003, Mar. 2024, https://doi.org/10.1016/j.aggp.2023.100003
-
Y. Deng, K. Zhang, J. Zhu, X. Hu, and R. Liao, “Healthy aging, early screening, and interventions for frailty in the elderly,” BioScience Trends, Vol. 17, No. 4, pp. 252–261, Aug. 2023, https://doi.org/10.5582/bst.2023.01204
-
E. Silva and L. H. R. Souza, “Acute effect of isometric handgrip exercise on blood pressure in elderly hypertensive individuals,” (in Portuguese) in Pathways to Longevity: Research on Aging and Physical Activity in the Interior of Bahia, Salvador, Brazil: Editora Omnis Scientia, 2025, pp. 86–95.
-
“Reducing social isolation and loneliness among older people,” World Health Organization, Geneva, Switzerland, 2025.
-
E. Courtin and M. Knapp, “Social isolation, loneliness and health in old age: A scoping review,” Health and Social Care in the Community, Vol. 25, No. 3, pp. 799–812, 2017, https://doi.org/10.1111/hsc.12311
-
“Social isolation and loneliness in older adults: Opportunities for the health care system,” National Academies Press, Washington, D.C., 2020, https://doi.org/10.17226/25663
-
A. Shvedko, A. C. Whittaker, J. L. Thompson, and C. A. Greig, “Physical activity interventions for treatment of social isolation, loneliness or low social support in older adults: A systematic review and meta-analysis of randomised controlled trials,” Psychology of Sport and Exercise, Vol. 34, pp. 128–137, Jan. 2018, https://doi.org/10.1016/j.psychsport.2017.10.003
-
A. R. Teo et al., “Effect of telehealth yoga on loneliness and social isolation among rural older adults: A randomized controlled trial,” Aging and Mental Health, Vol. 29, No. 5, pp. 824–832, 2025, https://doi.org/10.1080/13607863.2024.2449126
-
J. Holt-Lunstad, T. B. Smith, M. Baker, T. Harris, and D. Stephenson, “Loneliness and social isolation as risk factors for mortality: A meta-analytic review,” Perspectives on Psychological Science, Vol. 10, No. 2, pp. 227–237, 2015, https://doi.org/10.1177/1745691614568352
-
A. Liberati et al., “The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration,” BMJ, Vol. 339, No. jul21 1, pp. b2700–b2700, 2009, https://doi.org/10.1136/bmj.b2700
-
J. Higgins et al., Cochrane Handbook for Systematic Reviews of Interventions. Chichester, U.K.: John Wiley & Sons, 2023.
-
C. J. Gust, R. Martin-Willett, L. P. Gibson, G. Giordano, D. R. Seals, and A. D. Bryan, “Effects of aerobic exercise of different intensities on the social, emotional, and financial functioning of healthy older adults: results from a 16-week exercise randomized control trial,” GeroScience, Vol. 48, No. 1, pp. 391–403, 2025, https://doi.org/10.1007/s11357-025-01655-0
-
L. Nettlefold, H. M. Macdonald, J. Sims Gould, A. Bauman, Z. Szewczyk, and H. A. Mckay, “Does optimizing Choose to Move-a health-promoting program for older adults-enhance scalability, program implementation and effectiveness,” International Journal of Behavioral Nutrition and Physical Activity, Vol. 21, No. 1, 2024, https://doi.org/10.1186/s12966-024-01649-9
-
A. Gen et al., “Intervention for social frailty focusing on physical activity and reducing loneliness: A randomized controlled trial,” Clinical Interventions in Aging, Vol. Volume 20, pp. 43–53, Jan. 2025, https://doi.org/10.2147/cia.s491979
-
A. Zengin Alpozgen, K. Kardes, E. Acikbas, F. Demirhan, K. Sagir, and E. Avcil, “The effectiveness of synchronous tele-exercise to maintain the physical fitness, quality of life, and mood of older people: A randomized controlled study,” European Geriatric Medicine, Vol. 13, No. 5, pp. 1177–1185, 2022, https://doi.org/10.1007/s41999-022-00672-y
-
C. A. Jones et al., “Walk, talk and listen: A pilot randomized controlled trial targeting functional fitness and loneliness in older adults with hearing loss,” Open, Vol. 9, No. 4, p. e026169, 2019, https://doi.org/10.1136/bmjopen-2018-026169
-
C. Mastrogiovanni et al., “MovingTogether: A randomized controlled trial of a mental-health-informed digital health promotion intervention for older adults,” Age and Ageing, Vol. 54, No. 7, 2025, https://doi.org/10.1093/ageing/afaf190
-
World Health Organization, “Physical activity,” in World Health Organization, New York: World Health Organization, 2024, pp. 96–109, https://doi.org/10.4324/9780429323553-8
About this article

The authors have not disclosed any funding.
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Margarida Rocha: conceptualization, data collection, statistical analysis, data interpretation, and writing-original draft preparation. Beatriz Sousa: investigation and writing-review and editing. João Ribeiro: investigation and writing-review and editing. Samuel Campos: Investigation and writing-review and editing. Vitor Vinagre: investigation and writing-review and editing. Jorge Moreira: investigation and writing-review and editing. Alexandra Malheiro: supervision and writing-review and editing. Pedro Afonso: supervision and writing-review and editing. All authors have read and approved the final version of the manuscript.
The authors declare that they have no conflict of interest.
