Abstract
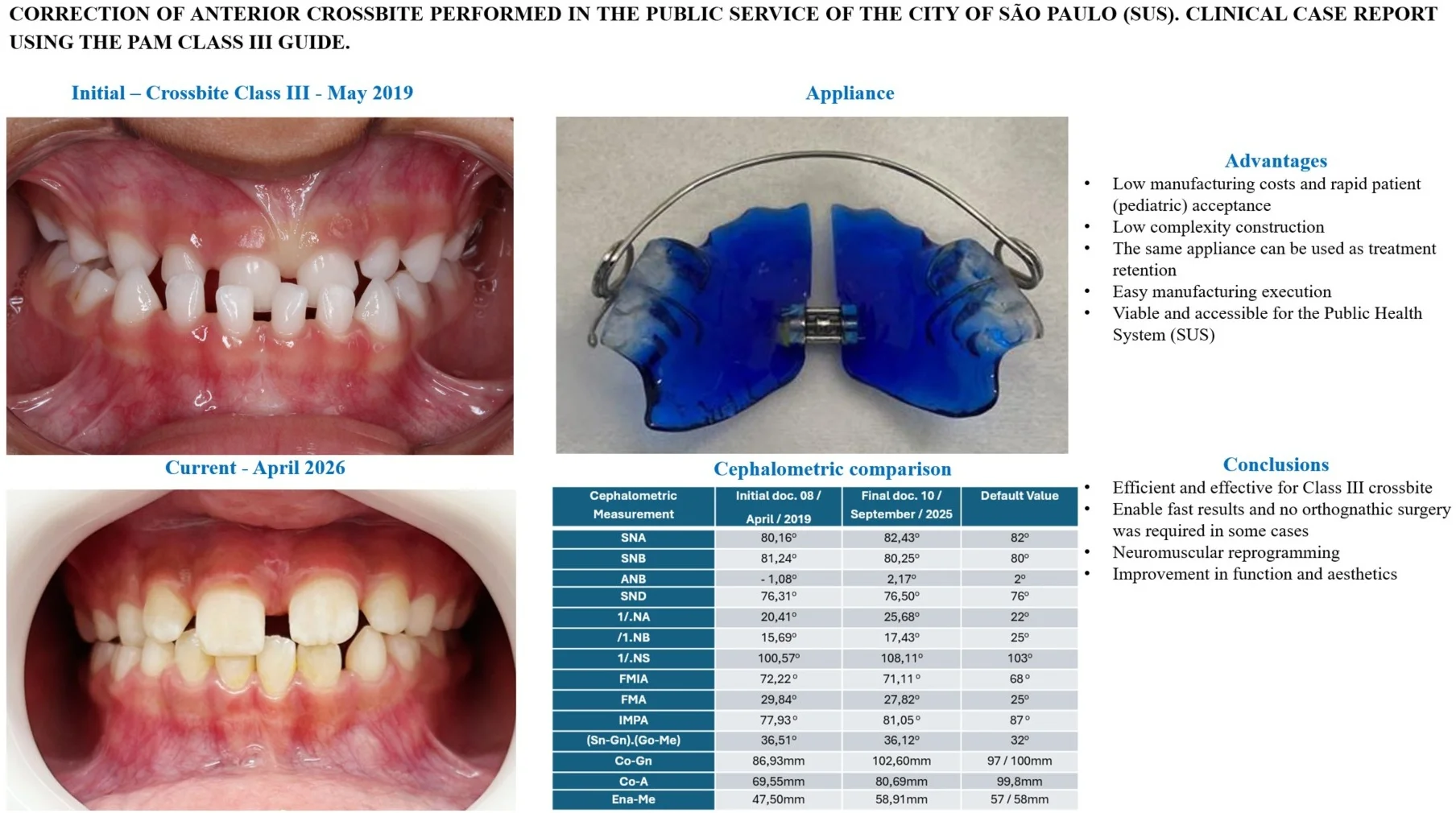
This clinical case report examines the efficacy of the GUIA PAM III (Marinho’s Posterior-Anterior Guide), a functional jaw orthopedic appliance, in treating Angle Class III malocclusion with anterior crossbite. The study focuses on a 3-year-old male patient treated within the Brazilian public health system (SUS), presenting with functional mandibular projection and deleterious parafunctional habits. The PAM III appliance was selected for its cost-effectiveness, high patient acceptance, and its unique design that eliminates the need for a constructive bite registration, which is particularly beneficial for very young patients. Treatment objectives centered on promoting therapeutic postural changes and neuromuscular reprogramming to stimulate maxillary growth while controlling mandibular development. Over the clinical follow-up period, bioprogressive activations were utilized to achieve balanced stomatognathic function and a harmonious facial profile without exerting excessive pressure on the dental arches. Cephalometric analyses post-active treatment revealed significant improvements, including an increase in the ANB angle and successful correction of the crossbite, effectively avoiding the need for future orthognathic surgery. The results demonstrate that the GUIA PAM III is a highly effective, comfortable, and simple tool for interceptive orthopedic intervention in growing patients.
1. Introduction
Human facial characteristics hold significant importance for individuals. Facial harmony and the structures supporting it are invariably noticed when discordant aspects are observed in an individual, influencing personality, extroversion, and sociability. Malocclusions directly or indirectly affect facial harmony, a subject that has been studied for a long time and was described as early as 1899 by Angle.
An epidemiological survey conducted in 2002 by Capelozza Filho in the region of Bauru, São Paulo, Brazil, found a prevalence of approximately 3 % for Class III malocclusion. This rate follows Japan, which has approximately 4 to 5 % of the population, but is higher than Europe, which presents a prevalence between 1 and 2 % [1].
The diagnosis of Class III malocclusion is characterized by a facial deformity originating from the patient's skeletal structure. Ideally, the diagnosis should be performed during the growth phase and is based on deviations in craniofacial development. Studies show that mandibular growth is predominantly endochondral in the condylar cartilage and is of genetic origin [2].
The combination of bone, dental, and muscular structures was analyzed by Araujo et al. (2023). The authors consider Class III malocclusion to be one of the most complex to treat [3].
The functional orthopedic appliance known as the Marinho Posterior-Anterior or Anterior-Posterior and Latero-Lateral Guide commonly referred to as the GUIA PAM was developed by Dr. Alfeu Vitelli Marinho Filho in 1968, based on observations of Bimler, Bionator, Planas, and Fränkel functional appliances. The PAM enables rapid results through therapeutic postural changes, supporting proper dental arch development via bioprogressive activations [4].
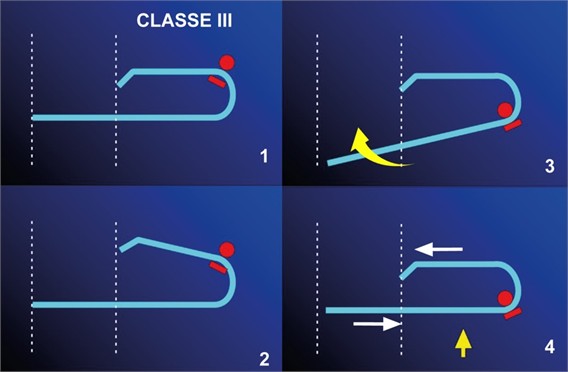
The appliance promotes balance within the stomatognathic system through stimuli, resulting in a harmonious facial profile and adequate masticatory function. In activations for Class III cases, the archwire does not exert pressure; it is adjusted only to regain a 'presence' touch on the cervical third of the mandibular incisors and canines, preventing the tipping of these teeth. During monthly follow-ups, it may be observed that the archwire has become loose and slightly away from the teeth; thus, it is adjusted through activations to achieve a subtle touch without exerting pressure. Alfeu Marinho refers to this type of activation as Bioprogressive (DAGHLIAN-2016). One way to facilitate the understanding of this activation, whether for Class II or III, is to open the end of the larger curve on the shorter arm of the archwire and close the end of the curve on the longer arm (Fig. 1).
Fig. 1Activations of the PAM III arch: Open the upper portion by 2 mm and close the lower portion, bringing the arch to parallelism
An example of the application of the GUIA PAM III for the treatment of Class III malocclusion can be observed in the article published by Marinho et al. (2025), in which the authors report a successful case of a patient with Class III malocclusion treated using the GUIA PAM (Postero-Anterior Marinho). In the article, the authors describe that the patient began treatment at 6 years and 8 months of age to reposition and control mandibular growth and correct the crossbite. Treatment began on August 11, 2021, with the initial orthodontic documentation and cephalometric measurements, aiming to compare them with the final stage of treatment and thus evaluate its effectiveness. The appliance was installed on January 10, 2022, along with usage instructions provided to the patient and guardian. The main recommendation was that the child should wear the appliance between 14 and 16 hours per day. After approximately 12 months, a new evaluation was performed together with updated documentation to assess the progress of treatment. Cephalometric analyses revealed significant changes: the SNA value, initially 84.54°, increased to 86.46°, and the 1/NA, initially 7.72°, increased to 17.14°. In the patient’s evaluation, expressive results were observed in a short period of time. The crossbite was corrected, and the occlusion proved to be stable and functional. The case study also highlighted the increase in the ANB angle, with mandibular repositioning combined with maxillary advancement. Conclusively, according to the authors, early use of the GUIA PAM III can bring effective improvements in occlusion and in the stomatognathic system, making it more functional. The appliance, according to the authors, is a simple and applicable solution for the functional orthopedic correction of Class III malocclusion [5].
2. Clinical case description
The treatment took place at the Dental Specialties Center (CEO) of the São Paulo municipal government. This is a service provided by the SUS (Unified Health System) for pediatric dental care in high-complexity cases. The patient, A.F.O.C. (3 years and 11 months old), was seen on April 2, 2019, presenting a diagnosis of Angle Class III malocclusion with a posterior crossbite. During the anamnesis, the patient’s mother reported that the child had a habit of resting his hand under his chin, causing the mandible to project forward. In addition to this deleterious habit, the patient also frequently slept with his hand resting on the right side of his face. The initial diagnosis considered treatment with Functional Jaw Orthopedics (FJO) for Class III correction, aiming to avoid future orthognathic surgery. The patient’s mother was advised on the necessity of eliminating these deleterious parafunctional habits for the success of the treatment. The patient was then referred for orthodontic records. The treatment plan was established in May 2019 in conjunction with the patient's guardian (mother), who reported progress in the cessation of deleterious habits. Impressions of both arches were taken, along with a habitual bite registration using number 7 wax.
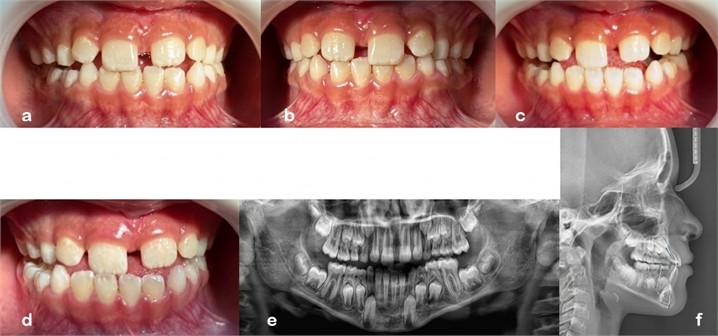
Fig. 2GUIA PAM III Appliance: a) Frontal extraoral photograph; b) lateral extraoral photograph; c) extraoral frontal photograph of a smiling face; d) intraoral photograph of the right side; e) frontal intraoral photograph; f) intraoral photograph of the left side; g) panoramic radiograph; h) lateral cephalometric radiograph; i) occlusal view of the appliance with central expansion screw



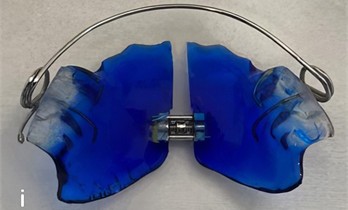
The Class III PAM Guide was the functional orthopedic appliance selected for the treatment, as it is easy to manufacture and well-accepted by patients. The expansion screw of the appliance was activated in the dental office by the orthodontist. Furthermore, it eliminates the need for a constructive bite registration, which would have been difficult to obtain given the patient's young age. And initial orthodontic documentation (Fig. 2).
Treatment began in June 2019 with the installation of the Class III PAM appliance. At the September follow-up visit of the same year, improvement in the bilateral crossbite was observed. During the March 2020 appointment, impressions of both arches were taken, along with a new wax bite registration, to fabricate a new appliance necessitated by the patient's transition to permanent dentition. Starting in April 2020, clinical appointments were interrupted due to the COVID-19 lockdown. The new appliance was not installed until July 20, 2020. At the December 2021 follow-up, correction of the anterior crossbite was observed, as shown in Fig. 3.
Fig. 3Intraoral photograph with appliance (April, 23, 2021): a) intraoral photograph of the right side; b) frontal intraoral photograph; c) intraoral photograph of the left side

In December 2021, the continuation of the treatment was authorized as it was a Class III case with potential for future orthognathic surgery, given that only treatments with a 24-month duration are permitted. During this visit, a new impression was taken for the fabrication of a new Class III PAM (Mandibular Protraction Appliance) tailored to the current stage of treatment. In the February consultation, the need for a superior labial frenectomy was also identified, which was performed on February, 23, 2022. The new appliance (Fig. 4) was installed in June 2024, featuring the addition of a doble cantilever spring on the palatal aspect of tooth 21 for labial tipping (vestibularization).
Between July and November 2024, new activations were performed according to the treatment plan, the expansion results already achieved, and the patient’s compliance with appliance wear. In September 2024, an improvement in the positioning of upper left central incisor (FDI 21) was observed. Extraoral photographs (Fig. 5(a, b)) from April 2025 and intraoral photographs (Fig. 5(c-f)) including right lateral, left lateral, and frontal views demonstrate the efficacy of the PAM Appliance in Class III treatment. The patient is currently using this appliance as retention, and follow-up appointments have been scheduled at longer intervals (every two months) for minor adjustments to the Class III PAM arch and the expansion screw, according to the patient’s growth and dental transition (mixed dentition).
Fig. 4GUIA PAM III appliance: a) intraoral photograph front view; b) photograph of the appliance with the addition of a doble cantilever spring in the region of tooth 21

Fig. 5Extraoral and Intraoral photograph (April, 17, 2025): a) frontal extraoral photograph; b) lateral extraoral photograph; c) frontal intraoral photograph; d) intraoral photograph of the left side; e) intraoral photograph of the right side; f) intraoral photograph with the appliance in place

The photographic records obtained in the dental office in September 2025 demonstrate the occlusal functionality and mandibular movements in habitual occlusion, as well as protrusive and right/left lateral excursions (Fig. 6), and the last photographs taken on April 1, 2026 (Fig. 7).
3. Discussion
The results of this clinical case demonstrate that early intervention with the GUIA PAM III (Posterior Anterior Marinho’s) is an effective strategy for correcting anterior crossbite in very young patients. The prevalence of this malocclusion in Brazil is approximately 3 % a significant figure that requires efficient, low-cost solutions, especially within the public health system (SUS). The fact that the device is low-cost, easily accepted, and easy to manufacture is extremely important for making treatment viable in public services and in developing countries. It can be offered to more patients at a lower cost.
Table 1Results of the initial and final cephalometric analyses of the active phase of treatment, demonstrating the benefits of treatment with Guia PAM III appliance
Cephalometric measurement | Initial doc. 08 / April / 2019 | Final doc. 10 / September / 2025 | Default value |
SNA | 80.16° | 82.43° | 82° |
SNB | 81.24° | 80.25° | 80° |
ANB | --1.08° | 2.17° | 2° |
SND | 76.31° | 76.50° | 76° |
1/.NA | 20.41° | 25.68° | 22° |
/1.NB | 15.69° | 17.43° | 25° |
1/.NS | 100.57° | 108.11° | 103° |
FMIA | 72.22° | 71.11° | 68 o |
FMA | 29.84° | 27.82° | 25° |
IMPA | 77.93° | 81.05° | 87° |
(Sn-Gn).(Go-Me) | 36.51° | 36.12° | 32° |
Co-Gn | 86.93 mm | 102.60 mm | 97 / 100 mm |
Co-A | 69.55 mm | 80.69 mm | 99.8 mm |
Ena-Me | 47.50 mm | 58.91 mm | 57 / 58 mm |
Fig. 6Functional intraoral photographs with mandibular movements: a) intraoral photograph with left lateral mandibular movement; b) intraoral photograph in habitual occlusion; c) intraoral photograph with right lateral mandibular movement; d) intraoral photograph with protrusive movement; e) panoramic radiograph; f) lateral cephalometric radiograph
A key finding in this study was the significant improvement in skeletal relationships, evidenced by the change in the ANB angle from -1.08° to 2.17°. This highlights the therapeutic shift characteristic of functional orthopedic treatment of the jaws. This shift indicates a successful transition from a Class III skeletal pattern to a Class I, effectively harmonizing the relationship between the maxilla and mandible. The increase in the SNA angle (from 80.16° to 82.43°) further supports the appliance's efficacy in stimulating maxillary growth, a critical objective in interceptive orthopedics. These findings align with previous studies, which obtained an initial SNA cephalometric measurement of 84.54° and a final measurement of 86.46°, while the ANB increased from 1.73° to 4.62° by Marinho et al. [5], which also observed significant improvements in SNA and 1/.NA values following PAM III therapy. In this clinical case, we observed that the 1/NA cephalometric measurement increased from 20.41° to 25.68°, indicating a labial tipping of the upper incisor crowns and an overall improvement of the case. This result is consistent with the findings of Marinho et al. [5], who reported a similar change from 7.72° to 17.14°.
Fig. 7Extraoral and Intraoral photograph (April, 01, 2026): a) lateral right side extraoral photograph; b) lateral left side extraoral photograph; c) intraoral right side photograph with the appliance; d) intraoral left side photograph with the appliance; e) intraoral photograph of the right side; f) frontal intraoral photograph; g) intraoral photograph of the left side

The unique design of the PAM III appliance offers several clinical advantages like constructive bite registration: Unlike many functional appliances, the PAM III eliminates the need for a complex constructive bite registration. The bioprogressive activations that use of “presence” touch rather than heavy pressure on the mandibular incisors prevented unwanted dental tipping while allowing for neuromuscular reprogramming. Patient compliance and cost: The low manufacturing cost and high comfort level facilitated patient adherence, which is vital for success in the public health sector.
Early diagnosis and treatment were paramount in avoiding the progression of the deformity. By correcting the functional mandibular projection and eliminating deleterious habits early, the treatment successfully avoided the need for highly invasive and costly orthognathic surgery in the future.
Although this case study highlights the effectiveness of the PAM III GUIDE, the results are limited to a single clinical report. Other research has been conducted previously with a larger sample size of patients, but more research is needed to confirm the stability of these results and to better explore the mechanics of the device in various clinical scenarios.
4. Conclusions
The recommended treatment proved to be both efficient and effective, as evidenced by the case records and the comparison of clinical photographs. This was further supported by the results of the McNamara cephalometric analysis conducted at the beginning of treatment (April 2019) and at the current stage (November 2025), successfully avoiding orthognathic surgery. The Class III GUIA PAM appliance presents itself as a viable alternative for the treatment of Class III patients within the public health system.
Functional Jaw Orthopedics (FJO) has evolved significantly, and the application of the new techniques presented in this article demonstrates their feasibility within the public health system. Low costs and rapid patient acceptance, combined with patient compliance regarding appliance wear and activation frequency, enable fast results that improve self-esteem and promote changes in therapeutic posture. Mandibular advancement or retrusion activations should be performed as follows: for Class II cases, mandibular advancement should be done in 2 mm increments, averaging once per month. For Class III cases, activations should preferably be carried out in monthly cycles, provided the recommended wear time is observed. In these appliances, the arch wire is not activated to exert pressure on the dental arch; instead, it is adjusted only to maintain “presence” contact with the mandibular incisors and canines at the cervical third, thereby preventing tipping of these teeth.
The GUIA PAM III device has a low manufacturing cost, generates little discomfort for the patient during use, and is easy to use, manufacture, and handle. The study showed the importance of identifying malocclusion, diagnosing and treating Class III malocclusion early, demonstrating clinical success in the planned interceptive and functional orthopedic treatment of the jaws, avoiding aggravations, the need for future treatments, and greater difficulties in subsequent interventions.
Successfully avoiding orthognathic surgery to date. But the certainty of maintaining this result can only be confirmed after the end of pubertal growth, where the Guia PAM itself can be used as a retainer.
Even achieving a satisfactory result in the case presented, more studies using this type of mechanics are necessary.
Both orthodontic documentation procedures were performed at the same dental radiology clinic (Oral x), located in São Paulo, Brazil. The 2019 documentation procedure was performed using a Vatech Pax 400. The 2025 documentation procedure was performed using Carestream. The software used for the cephalometric tracing was Proradis.
References
-
L. Capelozza F. et al., “Treatment of Class III: reviewing the method (ERM and traction) through a clinical case,” (in Portuguese), Dental Press Journal of Orthodontics and Facial Orthopedics, Vol. 7, No. 6, pp. 99–119, Nov. 2002.
-
P. V. P. Oltramari, D. G. Garib, A. C. C. F. Conti, J. F. C. Henriques, and M. R. Freitas, “Class III orthopedic treatment in distinct facial patterns,” (in Portuguese), Revista Dental Press de Ortodontia e Ortopedia Facial, Vol. 10, No. 5, pp. 72–82, Oct. 2005, https://doi.org/10.1590/s1415-54192005000500008
-
E. C. V. Araújo, E. D. S. Bronzi, J. M. A. Vera, L. S. Ferreira, and S. P. Brito, “Early treatment of Class III in a child patient,” (in Portuguese), Research, Society and Development, Vol. 12, No. 3, p. e17612340591, 2023, https://doi.org/10.33448/rsd-v12i3.40591
-
E. A. S. Serrano et al., Orthodontics and Orthopedics. (in Portuguese), Nova Odessa – SP- Brasil: Ed. Napoleão, Coleção APDESP, 2016.
-
R. Ribeiro Marinho, L. de Freitas Daghlian, F. Rodrigues Marinho, and V. Rodrigues Marinho, “Anterior crossbite treatment with Guia pam III appliance: a clinical case report,” Jaw Functional Orthopedics and Craniofacial Growth, Vol. 5, No. 2, pp. 37–44, Dec. 2025, https://doi.org/10.21595/jfocg.2025.24668
About this article

The authors have not disclosed any funding.
To the scientist and doctor ALFEU VITELLI MARINHO FILHO in memoriam.
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Maria Fernanda Mauro Boschi: conceptualization, data curation, project administration, supervision, visualization, writing-original draft preparation, writing-review and editing. Leon de Freitas Daghlian: conceptualization, data curation, investigation, methodology, project administration, resources, writing-original draft preparation, writing-review and editing. Rodolfo Ribeiro Marinho: conceptualization, data curation, writing-original draft preparation, writing-review and editing. Cidney Cato: conceptualization, data curation, software, writing-original draft preparation, writing-review and editing. Vinicius Marinho: final review.
The authors declare that they have no conflict of interest.
The research met all applicable standards for the ethics of experimentation. According to resolution No. 466, there is no need for approval of the research by the ethics committee. Participants provided written informed consent prior to the study.
