Abstract
Posterior crossbite (PCB) is a common malocclusion and its diagnosis must be careful, because only knowing its etiology can determine the treatment plan. The PCB can be dental, skeletal or functional. For each subtype, there is a specific treatment. The aim of this study was to report the treatment of two patients with Skeletal Unilateral Posterior Crossbite. The patients were treated with the same device, a Maurício expander with a Hawley arch. The technique employed, following the Knowledge of Jaw Functional Orthopedics (JFO), proved to be extremely efficient, allowing correction of crossbite malocclusion, mandible centralization, correct dental positioning, restoring conditions so that the growth and development of the patients occurred in a correct and balanced way.
1. Introduction
Posterior crossbite is characterized by the abnormal relationship, in the buccolingual direction, of one or more teeth in the maxilla, with one or more teeth in the mandible, in a centric relationship, which can be uni or bilateral [1]. The main etiologies of PCB are harmful oral habits, mouth breathing and orofacial muscle changes and the most common change in primary and mixed dentition [2]. Posterior functional crossbite is a common malocclusion in children, with a prevalence between 7.5-24 %. Different interventions have been used to correct this malocclusion, such as Planas Direct Tracks (PDT), which are an efficient treatment alternative for the primary dentition [3]. In mixed dentition, we have other alternative appliances to treat unilateral posterior crossbite [4], such as Simões Network appliances, encapsulated expanders and orthodontic devices. If this change is not treated, as a consequence, it may present asymmetry in the maxilla and mandible, changes in muscle electromyographic activity during chewing, changes in chewing movements, changes in swallowing and bite force [5-7].
Unilateral posterior crossbite can cause changes in the chewing cycle [8], studies show that environmental and functional factors interfere with craniofacial development [9]. As the PCB develops during the eruption of the primary dentition, it influences the development of central motor control, establishing the type of reverse sequencing chewing pattern [10]. In the absence of effective treatment, a serious functional asymmetry is established, which can lead to skeletal asymmetries, irreversible when maturity is reached [11] Recent studies show the possible relationship between mandibular deviation and the postural system [12, 13]. Therefore, the objective of this work was to report two clinical cases of unilateral posterior dentoalveolar crossbite with transvesal discrepancy between the arches, in two girls, aged 6 and 8 years, mixed dentition, initially treated with the same encapsulated expander device developed by Maurício Vaz de Lima [14], whose aim was to expand the maxilla, centralize the jaw, seeking balance of occlusion and chewing cycles.
2. Methodology
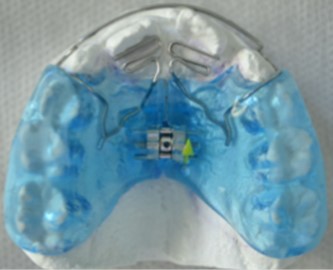
This work reports two clinical cases of unilateral posterior dentoalveolar crossbite with transvesal discrepancy between the arches by clinical analysis and study models, with a 6-year-old girl and an 8-year-old girl, with mixed dentition, treated with Maurício apparatus (Fig. 1).
Fig. 1Appliance similar to those used by the patients in this study
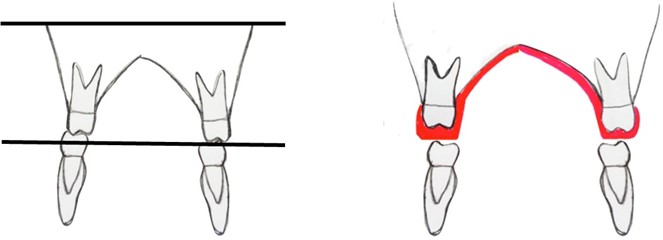
The two patients received the same protocol for time of use and activation of the appliance: time of use: during the night and 4 hours a day (1 hour in the morning, 1 hour after lunch, 2 hours in the late afternoon and for to sleep). Activation was ¼ turn once a week. This appliance was developed by Maurício Vaz de Lima [14], where adjustments were made to the encapsulated surface to achieve jaw alignment during use of the device, as shown in Fig. 2. Both patients preferred to chew on the side of the crossbite, and the occlusal plane was inclined, where the minimum vertical dimension was on the crossed side.
Fig. 2Schematic drawing showing the difference in thickness of the encapsulation to compensate for the inclination of the occlusal plane in relation to the Camper Plane
2.1. Case 1
Female patient, 6 years and 9 months old, preference for soft foods, maxillary atresia, unilateral crossbite on the right side, mandibular deviation to the right, distocclusion, lack of space for dental alignment (Figs. 3(a-d)). The jaw dynamics were altered, with masticatory preference on the right side. When closing the mouth, the first contact was obtained in centric occlusion and the mandible was diverted until functional occlusion was achieved. The cephalometric tracings requested were: Lavergne / Petrovic, McNamara, Bimler and USP analysis (Fig. 3(e)). Cephalometric analysis (Table 1) convex profile, mesocephalic, distocclusion, protruded maxilla, Petrovic category 1 P2DOB.
Fig. 3Initial intra-oral photographs of a) the right side, b) front, c) left side. Patient with Unilateral PCB, absence of teeth 11, 31 and 41. Half-erupted tooth 22 and distocclusion. Initial radiographic examination with d) panoramic radiograph, e) lateral cephalogram

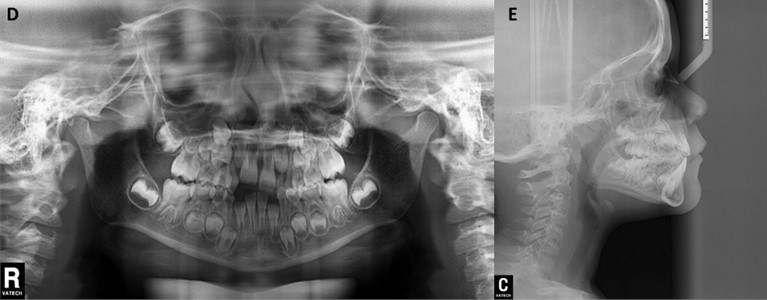
Table 1USP standard cephalometric measurements of the patient
Measurements | Standard | Value Obtained | Interpretation |
SNA | 82° +/-2° | 85.25° | Protruded maxilla |
SNB | 80° +/-2° | 79.10° | Well-positioned mandible |
ANB | 2° +/-2° | 6.14° | Skeletal class ii |
NAP | 0° a 2° +/-2° | 13.33° | Convex profile |
1.NA | 22° +/-0.5° | 17.24° | Upright upper incisors |
1-NA | 4 mm +/-0.5 mm | –0.24 mm | Retruded upper incisors |
1.NB | 25° +/-0.5° | 32.72° | Proclined lower incisors |
1-NB | 4 mm +/-0.5 mm | 4.04 mm | Well positioned lower incisors |
1.1 | 131° +/-0.5° | 123.89° | Convex profile |
FMA | 25° +/-5° | 28.53° | Mesofacial |
SN.Gn | 66° +/-5° | 65.18° | Mesofacial |
SN.Plo | 14°+/-0.5° | 20.52° | Divergent occlusal plane |
SN.GoGn | 32°+/-3° | 32.7° | Mesofacial |
Nasolabial | 10mm +/-1mm | 127.02° | Upper lip protrusion |
H-Nariz | 15° e 30° | 0.36 mm | Convex profile |
Orofaringe | 13,5 +/-4.3 mm | 18 mm | Forward tongue, mouth breathing |
After the patient signed the Informed Consent Form, the treatment plan with the Maurício expander device was proposed. After molding and manufacturing the device, a new appointment was scheduled for the installation of the device. The patient was instructed to use the device for sleep and part of the day (Fig. 4). Activation: 1/4 turn weekly. After 7 months, to assist in the treatment, since the device is removable, selective grinding was carried out on the buccal cusp of 83 and it was observed that the dental occlusion resulted in centralization of the mandible. Subsequently, the acrylic was removed from elements 63 and 53 and a PDT was made on tooth 53 in composite resin were created centralizing the midline, where the correction crossbite and centralization of the mandible was observed (Fig. 5). After 10 months of starting treatment, it was possible to observe a significant improvement in the patient's occlusion. the correction of the unilateral MCP and remaining a slight midline deviation, however, after uncrossing the bite, Planas Indirect Tracks were installed. The patient continues to undergo treatment (Fig. 6).
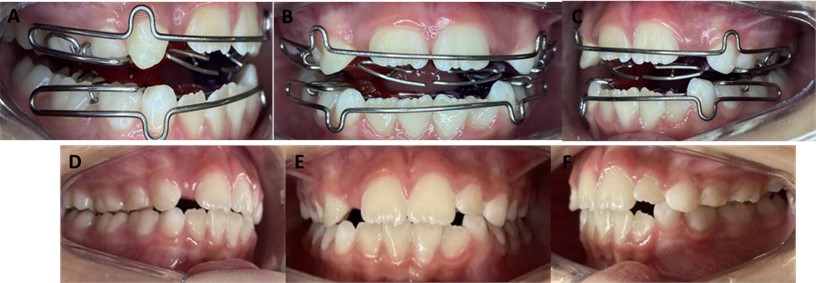
Fig. 4Installation of the apparatus Maurício expander with midline centering. Activation: 1/4 turn weekly. Intra-oral photographs of the a) right side, b) front, c) left side

Fig. 5Intra-oral photographs of the a) right side, b) front, c) left side, after 7 months of the treatment, with selective wear and PDP in the 53

Fig. 6Installation of the apparatus Planas Indirect Tracks. Activation: 1/4 turn months. Intra-oral photographs of the a) right side, b) front, c) left side. Final intra-oral photographs of the d) right side, e) front, f) left side, after 10 months of the treatment. The patient continues to undergo treatment
2.2. Case 2
Female patient, 8 years old, preference for soft foods, respiratory complaint of allergic rhinitis, maxillary atresia, unilateral crossbite on the left, mandibular deviation to the left, distocclusion, lack of space for dental alignment. Altered mandibular dynamics, with left chewing preference (Figs. 7(a-d)). The cephalometric tracings requested were: Lavergne / Petrovic, McNamara, Bimler and USP analysis (Fig. 7(e)). Cephalometric analysis: convex profile, mesocephalic, distocclusion, protruded maxilla and retruded mandible, Petrovic category 3 R2DOB (Table 2). After the patient signed the Informed Consent Form, the treatment plan with the Maurício expander device was proposed. After molding and manufacturing the device, a new appointment was scheduled for the installation of the device. The neuroclusal deprogramming promoted by the device made it possible to centralize the mandible. The patient was instructed to use the device for sleep and part of the day. Activation: 1/4 turn weekly. during treatment, occlusal adjustments were made. The patient was instructed to use the device for sleep and part of the day. (Figs. 8(a-c)). during treatment, occlusal adjustments were made. One month after installing the device, the acrylic was removed from the region of 53 and 63 and selective grinding was carried out on the mesio-palatal surface of 63 and on the distobuccal surface of 73. Subsequently, PDTs were created on 63, 53 and 83. After 7 months of starting treatment, it was possible to observe a significant improvement in the patient's occlusion (Figs. 8(d-f)). the correction of the unilateral MCP and remaining a slight midline deviation the patient will continue treatment with functional jaw orthopedics.
Fig. 7Initial intra-oral photographs of the a) right side, b) front, c) left side. Patient with Unilateral PCB, and distocclusion. Initial radiographic examination with d) panoramic radiograph, e) lateral cephalogram
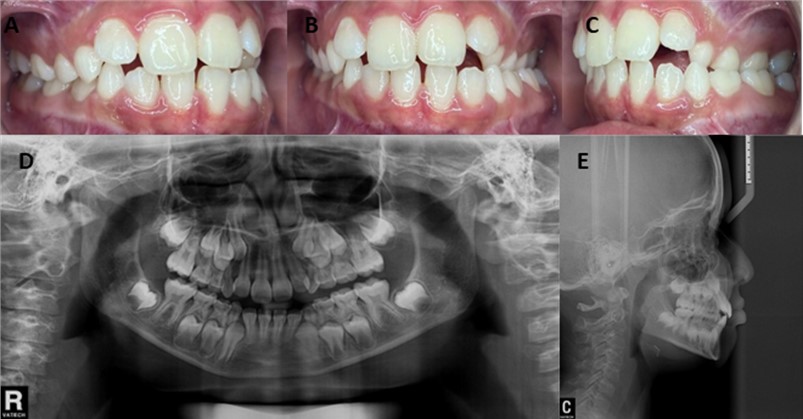
Table 2USP standard cephalometric measurements of the patient
Measurements | Standard | Value obtained | Interpretation |
SNA | 82° +/-2° | 84.84° | Protruding maxilla |
SNB | 80° +/-2° | 77.91° | Retruded mandible |
ANB | 2° +/-2° | 6.92° | Skeletal class ii |
NAP | 0° a 2° +/-2° | 13.17° | Convex profile |
1.NA | 22° +/-0,5° | 19.64° | Upright upper incisors |
1-NA | 4 mm +/-0.5 mm | 0.34 mm | Retruded upper incisors |
1.NB | 25° +/-0.5° | 25.90° | Well positioned lower incisors |
1-NB | 4 mm +/-0.5 mm+ | 9.44 mm | Protruded lower incisors |
1.1 | 131° +/-0.5° | 127.54° | Convex profile |
FMA | 25° +/-5° | 24.25° | Mesofacial |
SN.Gn | 66° +/-5° | 68.57° | Mesofacial |
SN.Plo | 14°+/-0.5° | 19.83° | Divergent occlusal plane |
SN.GoGn | 32°+/-3° | 33.86° | Mesofacial |
Nasolabial | 104,4° | 96.49° | Upper lip retrusion |
H-Nariz | 15° e 30° | 2.45 mm | Convex profile |
Orofaringe | 13,5 +/-4.3 mm | 12.31 mm | Well positioned tongue |
3. Discussions
This study presented two case reports with unilateral PCB treated with bilateral Mauritius expander and PDTs. PCB is a transverse malocclusion, which can be caused by maxillary atresia, mandibular atresia, premature contact, maxillary asymmetry, interference by external factors, such as harmful habits and mouth breathers [15, 16]. PCB treatment can be challenging depending on its classification [2, 17, 18]. Souza; Mucheli, Herdy [19], state that if PCB is not treated in the primary dentition, it may lead to occlusal, functional, aesthetic and TMJ dysfunctions. Deshayes [20] states that early treatment of malocclusions, aiming at complete symmetrization of the patient, restores conditions to protect them from late complications. Valério; Azevedo [21], reiterate saying that the fullness of functions only occurs with balance of the Stomatognathic System. Although the ages presented here were 6 and 8 years, during the mixed dentition, there was a good evolution, perhaps, if they were treated at a younger age, the results could be different, especially with regard to facial symmetrization.
Fig. 8Installation of the apparatus Maurício expander with midline centering obtained by adjusting the acrylic. Activation: 1/4 turn weekly. Intra-oral photographs of the a) right side, b) front, c) left side. Removal of the acrylic from the 53 and 63 region and carrying out selective grinding and creation of the PDTs, of the d) right side, e) front, f) left side. Final intra-oral photographs of the g) right side, h) front, i) left side, after 7 months of the treatment. the patient continues to undergo treatment

Sever; Marion; Ovsenik [22] state that PCB sufferers maintain unilateral chewing. Lima et al. [23] concluded, in their research, that there is no relationship between the consistency of the food ingested and the occurrence of MCP. in both cases (patient 1 and 2), there was a change in mandibular dynamics and a chewing preference on the side of the crossbite. Several types of treatment can lead to the resolution of this malocclusion, from simple removal of the harmful habit to the use of removable functional orthopedic appliances [17, 24]. Peña-Santana; Reyes-Castellanos; Telléz-Peña [25] declare that the success of the treatment depends not only on the device chosen, but also on the collaboration of the patient and parents, the origin of the malocclusion and the magnitude of the discrepancy presented.
PCB treatment, PDTs are found in the literature, which begins with selective wear and subsequently the manufacture of PDTs in composite resin [26, 27]. in one case report, the correction of the malocclusion was around 95 days after PDTs [26], however, another study corrected it after 29 days [28]. These time variations are due to each individual responding in a certain way, depending on genetics, age, sex and whether the patient is supportive of the treatment [26, 28]. Treatment with neuro-occlusal rehabilitation has proven effective in around 79 % of PCB cases [29].
Other therapies in evidence are removable encapsulated expanders, according to the treatment proposed by Silva et al. [30] who used removable encapsulated expanders with unilateral constructive bite, and observed occlusion resolution in 9 months and 12-month follow-up. in association, Brandão et al. [31] used a removable expander encapsulated with a Gomes flap over a period of 9 months to completely uncross the arches. Therefore, several techniques demonstrate the effectiveness of therapies promoted by OFM and Orthodontics in short and prolonged periods, both in AOB and MCP [2, 29]. Therefore, among the various treatment options in OFM, we opted for the Maurício Expander, Flat Direct Tracks and in the first patient, it ended with simple Flat Indirect Tracks to treat the PCBs and both patients collaborated with the treatment.
4. Conclusions
The techniques used proved to be efficient, enabling the correction of crossbite. After gaining transverse dimension and uncrossing the bite, this appliance is replaced by another functional orthopedic appliance without the encapsulation to continue stimulating therapeutic posture changes and allowing the development and achievement of balanced occlusion. The Jaw Functional Orthopedics has a large therapeutic arsenal that can be used at different times, according to the needs of each patient. for example, after this expansion phase with the device presented, the two patients were treated with Planas Indirect Tracks. Treatment should begin as soon as diagnosed, preferably in childhood so that the balance of jaw development occurs as soon as possible, avoiding greater damage in adulthood.
References
-
A. Locks et al., “Posterior crossbite: a more didactic classification,” (in Portuguese), Revista Dental Press de Ortodontia e Ortopedia Facial, Vol. 13, No. 2, pp. 146–158, Apr. 2008, https://doi.org/10.1590/s1415-54192008000200017
-
J. H. A. Cruz, E. R. L. Souza, L. X. Sousa, B. F. Oliveira, G. M. T. Guênes, and M. C. B. Macena, “Mordida cruzada posterior: um enfoque à epidemiologia, etiologia, diagnóstico e tratamento,” (in Portuguese), Archives Health Investigation, Vol. 8, No. 3, pp. 157–163, May 2019, https://doi.org/10.21270/archi.v8i3.3180
-
D. A. Lentini-Oliveira, “Planas direct tracks to treat functional crossbites in children: scientific evidence,” Jaw Functional Orthopedics and Craniofacial Growth, Vol. 2, No. 2, pp. 24–31, Nov. 2022, https://doi.org/10.21595/jfocg.2022.22739
-
W. A. Simões, Ortopedia Funcional dos Maxilares através da Reabilitação Neuro oclusal. (in Portuguese), Porto Alegre: Artes Médicas, 2003.
-
A. D. S. Andrade, M. B. D. Gavião, G. H. Gameiro, and M. Rossi, “Characteristics of masticatory muscles in children with unilateral posterior crossbite,” Brazilian Oral Research, Vol. 24, No. 2, pp. 204–210, Jun. 2010, https://doi.org/10.1590/s1806-83242010000200013
-
G. Iodice, G. Danzi, R. Cimino, S. Paduano, and A. Michelotti, “Association between posterior crossbite, skeletal, and muscle asymmetry: a systematic review,” the European Journal of Orthodontics, Vol. 38, No. 6, pp. 638–651, Jan. 2016, https://doi.org/10.1093/ejo/cjw003
-
A. S. Pinto, P. H. Buschang, G. S. Throckmorton, and P. Chen, “Morphological and positional asymmetries of young children with functional unilateral posterior crossbite,” American Journal of Orthodontics and Dentofacial Orthopedics, Vol. 120, No. 5, pp. 513–520, Nov. 2001, https://doi.org/10.1067/mod.2001.118627a
-
M. G. Piancino et al., “Effects of therapy on masseter activity and chewing kinematics in patients with unilateral posterior crossbite,” Archives of Oral Biology, Vol. 67, pp. 61–67, Jul. 2016, https://doi.org/10.1016/j.archoralbio.2016.03.013
-
J. L. Yu, A. Tangutur, E. Thuler, M. Evans, and R. C. Dedhia, “The role of craniofacial maldevelopment in the modern OSA epidemic: a scoping review,” Journal of Clinical Sleep Medicine, Vol. 18, No. 4, pp. 1187–1202, Apr. 2022, https://doi.org/10.5664/jcsm.9866
-
G. S. Throckmorton, B. H. Buschang, H. Hayasaki, and T. Phelan, “The effects of chewing rates on mandibular kinematics,” Journal of Oral Rehabilitation, Vol. 28, No. 4, pp. 328–334, Dec. 2001, https://doi.org/10.1046/j.1365-2842.2001.00679.x
-
J. Wu, J. S. Y. Bek, M. Luo, H. Xu, Y. Wang, and X. Han, “Three-dimensional quantitative analysis of dental and skeletal characteristics of skeletal Class I unilateral posterior crossbite in adults,” BMC Oral Health, Vol. 22, No. 1, pp. 1–11, Dec. 2022, https://doi.org/10.1186/s12903-022-02622-3
-
L. Cardinal, T. R. Da Silva, A. L. F. Andujar, B. F. Gribel, G. C. Dominguez, and N. Janakiraman, “Evaluation of the three-dimensional (3D) position of cervical vertebrae in individuals with unilateral posterior crossbite,” Clinical Oral Investigations, Vol. 26, No. 1, pp. 463–469, Jul. 2021, https://doi.org/10.1007/s00784-021-04020-5
-
M. G. Piancino, G. Matacena, U. Garagiola, F. B. Naini, A. Tortarolo, and D. Wertheim, “Association between posterior unilateral functional crossbite and asymmetrical spinal flexion: a prospective study,” Heliyon, Vol. 9, No. 3, p. e14342, Mar. 2023, https://doi.org/10.1016/j.heliyon.2023.e14342
-
V. L. Maurício and S. Humberto, Reabilitação Dinâmica Funcional dos Maxilares Sem Extração. (in Portuguese), Nova Odessa: Quintessence, 1994.
-
Pereira and M. B. B., Manual de Ortopedia Funcional dos Maxilares. (in Portuguese), Rio de Janeiro: Santos, 2017.
-
E. R. Batista and D. C. L. Dos Santos, “Mordida cruzada posterior em dentição mista,” (in Portuguese), Revista de Odontologia da Universidade Cidade de São Paulo, Vol. 29, No. 1, p. 66, Jan. 2017, https://doi.org/10.26843/ro_unicid.v29i1.198
-
F. A. Fabre, “Mordida aberta anterior – considerações-chave,” (in Portuguese), Archives Health Investigation, Vol. 3, No. 5, pp. 48–56, 2014.
-
I. D. P. Luna, P. M. Mourelle, L. T. Moreta, and B. B. Villar, “Early treatment of unilateral posterior cross bite in the child patient. Literature review,” Científica Dental, Vol. 13, No. 1, pp. 41–48, 2016.
-
B. Souza, E. Mucheli, and J. L. Herdy, “Mordida cruzada posterior na dentadura decídua e mista – uma revisão bibliográfica,” (in Portuguese), Revista Rede de Cuidados em Saúde, Vol. 10, No. 1, pp. 1–10, 2017.
-
M.-J. Deshayes, “Orthopedically treat asymmetries before the age of six or How to Symmetrize Craniofacial Growth and Optimize Functioning temporomandibular,” L’Orthodontie Française, Vol. 81, No. 3, pp. 189–207, Aug. 2010, https://doi.org/10.1051/orthodfr/2010021
-
P. Valério and A. E. B. I. Azevedo, “Crescimento e desenvolvimento Craniofacial: entre a tenra infância e a adolescência,” (in Portuguese) in Manual de Adolescencia, Barueri: Manole, 2019.
-
E. Sever, L. Marion, and M. Ovsenik, “Relationship between masticatory cycle morphology and unilateral crossbite in the primary dentition,” the European Journal of Orthodontics, Vol. 33, No. 6, pp. 620–627, Dec. 2011, https://doi.org/10.1093/ejo/cjq070
-
N. K. B. Lima, V. D. Correia, N. C. C. Alves, M. A. S. Da Figueira, A. M. Da Paz, and J. G. B. Medrado, “Evaluation of the influence of dietary pattern on the development of dental malocclusions: a descriptive cross-sectional observational study,” (in Portuguese), Revista Uningá, Vol. 56, No. S5, pp. 67–77, Jul. 2019, https://doi.org/10.46311/2318-0579.56.euj2898
-
B. C. D. Silva, D. C. L. D. Santos, E. Flaiban, D. Negrete, and R. L. D. Santos, “Anterior open bite: origin and treatment,” (in Portuguese), Revista de Odontologia da Universidade Cidade de São Paulo, Vol. 31, No. 1, p. 68, Aug. 2019, https://doi.org/10.26843/ro_unicidv3112019p68-73
-
Y. Peña-Santana, N. Reyes-Castellanos, and T. Telléz-Peña, “Tratamiento temprano de la mordida cruzada posterior con placas Hawley de expansión y elásticos cruzados,” (in Spanish), Revista Electrónica Dr. Zoilo E. Marinello Vidaurreta, Vol. 44, No. 6, 2019.
-
A. J. I. Garbin, B. Wakayama, T. A. S. Rovida, and C. A. S. Garbin, “The use of the direct plane track in the early treatment of posterior crossbite: case report,” (in Portuguese), Archives Health Investigation, Vol. 5, No. 4, pp. 182–185, Sep. 2016, https://doi.org/10.21270/archi.v5i4.1326
-
A. J. I. Garbin, B. Wakayama, R. R. Santos, T. A. S. Rovida, and C. A. S. Garbin, “Pistas diretas planas para o tratamento de mordida cruzada posterior,” (in Portuguese), Revista Cubana Estomatologia, Vol. 51, No. 1, pp. 113–120, 2014.
-
P. A. Vedoatto, B. Wakayama, C. A. S. Garbin, A. T. Saliba, and A. J. I. Garbin, “Reabilitação neuroclusal e a intervenção precoce na má oclusão: relato de 6 anos de acompanhamento,” (in Portuguese), Archives Health Investigation, Vol. 7, No. 3, p. 366, 2018.
-
A. J. I. Garbin, B. Wakayama, T. A. S. Rovida, and C. A. S. Garbin, “Neuroclusal rehabilitation and planas direct tracks in the posterior crossbite treatment,” (in Portuguese), Revista Gaúcha de Odontologia, Vol. 65, No. 2, pp. 109–114, Jun. 2017, https://doi.org/10.1590/1981-863720170002000023046
-
A. C. F. Silva, M. F. L. Silva, L. N. Silva, V. S. B. Cabral, and S. M. S. Silva, “Reabilitação neuroclusal no tratamento de mordida cruzada posterior unilateral em paciente pediátrico,” (in Portuguese), Archives Health Investigation, Vol. 7, No. 5, p. 185, 2018.
-
R. M. R. Brandão, P. L. Aguiar, L. N. Silva, R. R. Barros, and S. M. S. Silva, “Mordida cruzada unilateral em paciente infantil tratado com aparelho ortopédico funcional,” (in Portuguese), Archives Health Investigation, Vol. 7, No. 5, p. 103, 2018.
About this article

The authors have not disclosed any funding.
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Valéria Medau: conceptualization, data curation, investigation, methodology, literature review, writing-original draft preparation, writing-review and editing. Nayara Nery de Oliveira Cunha: investigation, methodology, writing-original draft preparation, writing-review and editing. Patrícia Braga Navarro: investigation, methodology, writing-original draft preparation, writing-review and editing. Luciano Aparecido de Almeida-Junior: literature review, writing-original draft preparation; writing-review and editing. Ana Paula Cunha Tortelli: supervision, methodology, writing-original draft preparation, writing-review and editing.
The authors declare that they have no conflict of interest.
The Informed Consent Form was presented and signed by those responsible.
