Abstract
The term plagiocephaly means oblique head. Most skull deformities are a result of intrapartum or utero molding but can be caused by congenital torticollis and after birth due to persistent head position of newborns staying in one head position for a long time and abusive use of strollers, car seats, car seats, swings. Its prevalence is growing fast, in 30 years it passes from 1 in each 300 babies in early nineties to 16 to 48 % in 2020. The aim of this paper is bringing the light to some serious conditions of treatment protocols in individuals with plagiocephaly. The skull deformity causes facial asymmetry that are not treatable by orthopedic or orthodontic intra or extra oral appliances, nor orthognathic surgery. Well, despite the fact that the patient or the tutors have to be notified of the facial asymmetry that persists, functional limitations will be presented. In more than 30 years of clinical experience treating these patients it was never sought the 4 first permanent molars and the 4 canines in the same Angle’s Class. In one side can be seen Class 1, but on the other it will be finding class 2 or class 3, the case reported exemplifies it, and the worst, mastication guidance will have to be very carefully done since, in most cases if it is tried to adjust the inferior and superior dental midline the vertical asymmetry of the occlusal plane (minimum vertical dimension) will worsen. Really there is no unique treatment protocol and it has to be considered case by case. It is time to deepen the knowledge in this area since the prevalence is growing. Based on the case reported, non-treated plagiocephaly can bring serious limitations to malocclusion treatment results. Further studies are necessary to a better understanding of the situation plagiocephaly versus malocclusion.
Highlights
- Individuals with Plagiocephaly demands special care in malocclusion treatment.
- Symmetry of the cranium must be observed when treating malocclusion.
- Due to the facial asymmetry caused by cranial asymmetry treatment of malocclusion in these cases have significant limitations.
1. Introduction
The term plagiocephaly is a Greek derivative meaning “oblique head”. Most skull deformities present at birth are the result of in utero or intrapartum molding. Associated conditions involve uterine constraint, especially in cases of multiple birth infants, and birth injury associated with forceps or vacuum-assisted delivery. Positional plagiocephaly is an asymmetrical deformity of the skull, which can be caused by several factors: childbirth, multiple births, preterm birth, and congenital torticollis [1]. According to Yung and Yun [2] positional plagiocephaly (PP) can be diagnosed mainly by clinical examination and physical examination and is defined as a deformity and flattening of one side of the head due to persistent posture. These deformation processes occur mainly in the first months of life. This is because newborns stay in one position for a long time. It can happen due to the abusive use of strollers, car seats, car seats, swings, among others.
Ellwood et al. [3] states that before 1992 the rate of deformities was estimated at 1 in 300 babies. Recently, PP rates range from 16 % to 48 % for typical healthy infants under 1 year of age, which may change depending on the diagnostic criteria used, and 37.8 % for infants aged between 8 and 12 weeks, and affects 40 % of typical health infants younger than 1 year [1]. Due to this increase in prevalence, there has been an increase in the interest in investigating, controlling and preventing this condition.
When diagnosing plagiocephaly, it is important to examine the upper part of the skull (Figs. 1 and 2), analyze the position of the ears and cheeks, if the mandible is deviated on the side where the frontal bone is flattened, with the chin deviated to the side of frontal bone flattening [1].
With the right information, PP can be corrected and prevented. Osteopathic physical therapy helps detect and treat postural plagiocephaly in its early stage. The primary treatments for plagiocephaly are non-surgical and include observation, repositioning of the head, manual therapy and, in more advanced and severe cases, cranial orthosis therapy [1-3].
The importance of understanding the relationship between plagiocephaly and dental malocclusion goes beyond aesthetic correction, as it can contribute to the promotion of healthy craniofacial development and to the improvement of the quality of life of children worldwide. The relationship between plagiocephaly and dental malocclusion is still a relatively recent and complex area of research, involving multiple anatomical, behavioral, and genetic factors. Understanding this connection could have significant implications for children's health, such as preventive orthodontics and short- and long-term treatment [4]. While aesthetic correction of the head may be a concern for parents, there is growing evidence that plagiocephaly may also influence the development of malocclusion.
2. Case report
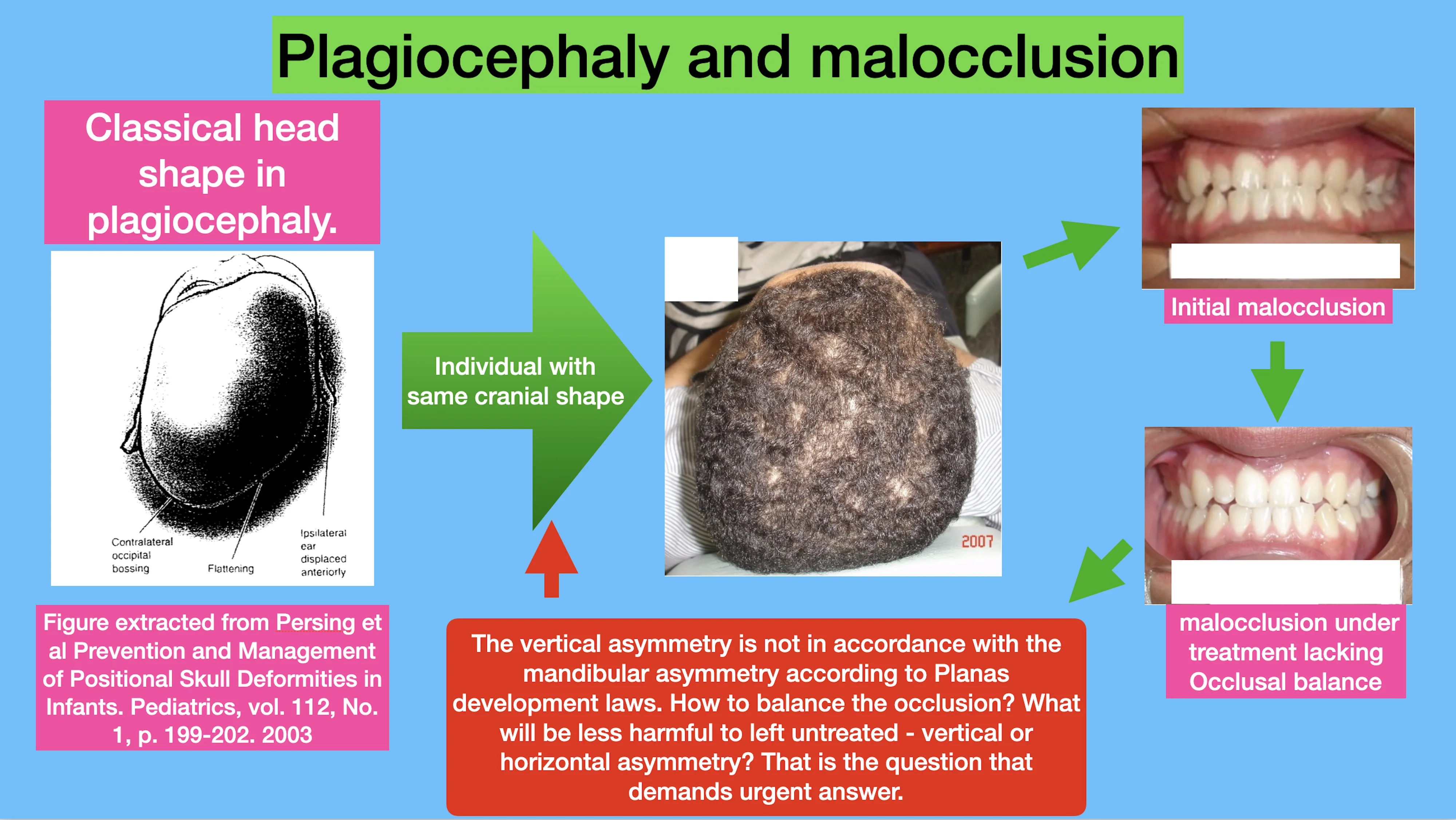
Through a case report it is intended to show how non treated plagiocephaly may compromise the malocclusion treatment final results due to the influence of plagiocephaly in facial symmetry and malocclusion. A 27 years old male patient with anterior cross bite searched for treatment. During the first examination severe facial symmetry was found. When examining the head of the patient a skull asymmetry was found (Fig. 1). Compare the head shape in figure one with Fig. 2 from Persing et al. [1] how similar it is. This shape tends to bring facial asymmetry not treatable with JFO or any oral device since it is due do cranial deformation. This is a valuable information for clinicians to talk about treatment possibilities and limitations with the tutors when the patient is underage or the individual when over age.
Fig. 1Top-down view of the individual cranium where can be noticed that the left side of the frontal bone is more posterior than the right

Fig. 2Classical head shape in plagiocephaly. Figure extracted from Persing et al. [1]
![Classical head shape in plagiocephaly. Figure extracted from Persing et al. [1]](https://static-01.extrica.com/articles/23860/23860-img2.jpg)
The intraoral examination showed an anterior cross bite and an inferior midline deviation do the left side (Fig. 3). In the frontal PA teleradiograph there was no mandibular deviation to the left side but the length of the mandible was greater on the right side, on Planas [5] gnatostathic sheet also no mandibular deviation to the left side were found. In the distance of the tragus on the right side to the sagittal plane is greater than the distance of the left tragus to, this can be seen in Fig. 1, on the right side the head is bulged. The first appliance prescript was a Simões Network 3 (SN3) (Fig. 5) functional orthopedic appliance [6] with progeny arch to guide and control mandibular position and a Planas Equiplan [5] to serve as a plateau for uncrossing the anterior bite. Frontal Springs were used to stimulate pre maxilla remodeling. After uncrossing the anterior bite, a Simões Network 7 (SN7) (Fig. 6) was prescript to balance and functionalize the occlusal plane. Laboratorial construction of the appliances can be seen at https://ohi-s.com/webinars-courses/167648/. On Fig. 4 the uncrossed anterior bite can be seen but the inferior midline deviation to the right persists.
Fig. 3Patient with anterior cross bite

Fig. 4Anterior bite uncrossed

Fig. 5Simões Network 3 – SN3 functional orthopedic appliance, at left frontal view and at right top-down view. Figure extracted from Santiago Jr. and Santiago 2010 [7]
![Simões Network 3 – SN3 functional orthopedic appliance, at left frontal view and at right top-down view. Figure extracted from Santiago Jr. and Santiago 2010 [7]](https://static-01.extrica.com/articles/23860/23860-img5.jpg)
![Simões Network 3 – SN3 functional orthopedic appliance, at left frontal view and at right top-down view. Figure extracted from Santiago Jr. and Santiago 2010 [7]](https://static-01.extrica.com/articles/23860/23860-img6.jpg)
Fig. 6Simões Network 7 – SN7 functional orthopedic appliance, at left frontal view and at right top-down view. Authors’ own figure. On the top occlusal view of superior and inferior appliances showing the Planas indirect tracks. On the middle frontal view of the appliance showing the buckle of the progeny arch with the clef arch. Bottom view showing the Planas indirect tracks and a lateral view of the buckle. Figure extracted from Santiago Jr. and Santiago 2010 [7]
![Simões Network 7 – SN7 functional orthopedic appliance, at left frontal view and at right top-down view. Authors’ own figure. On the top occlusal view of superior and inferior appliances showing the Planas indirect tracks. On the middle frontal view of the appliance showing the buckle of the progeny arch with the clef arch. Bottom view showing the Planas indirect tracks and a lateral view of the buckle. Figure extracted from Santiago Jr. and Santiago 2010 [7]](https://static-01.extrica.com/articles/23860/23860-img7.jpg)
![Simões Network 7 – SN7 functional orthopedic appliance, at left frontal view and at right top-down view. Authors’ own figure. On the top occlusal view of superior and inferior appliances showing the Planas indirect tracks. On the middle frontal view of the appliance showing the buckle of the progeny arch with the clef arch. Bottom view showing the Planas indirect tracks and a lateral view of the buckle. Figure extracted from Santiago Jr. and Santiago 2010 [7]](https://static-01.extrica.com/articles/23860/23860-img8.jpg)
![Simões Network 7 – SN7 functional orthopedic appliance, at left frontal view and at right top-down view. Authors’ own figure. On the top occlusal view of superior and inferior appliances showing the Planas indirect tracks. On the middle frontal view of the appliance showing the buckle of the progeny arch with the clef arch. Bottom view showing the Planas indirect tracks and a lateral view of the buckle. Figure extracted from Santiago Jr. and Santiago 2010 [7]](https://static-01.extrica.com/articles/23860/23860-img9.jpg)
3. Discussion
This view angle in Fig. 1 is becoming more and more necessary, due to the large increase in incidence of plagiocephaly, in the diagnosis session of individuals with facial asymmetry who look for treatment with jaw functional orthopedics. On the other hand, this problem will increasingly strengthen the relationship of dentistry and physiotherapy in treatment of facial asymmetry at the same time that it brings to light the much-discussed topic of early treatment.
There never will be early treatment, in our humble opinion, what happens frequently is the use of incorrect treatment protocol that leads to a longer treatment, but, by the time the facial asymmetry and/or the malocclusion is diagnosed there is a need for intervention to avoid worsening of the problem and bring more limitations to the final result of the treatment. The child must be taken to a dental office within the first 2 months of life to a craniofacial exam and breastfeeding guidance.
For sure there are many other cranial deformities, some made on purpose for religion or cultural reasons. We intend in this editorial letter to attract attention of the clinicians to observe more the cranium of the patient when diagnosing malocclusion to elaborate a more accurate treatment planning and expected results mainly when dealing with facial asymmetry or neck and head pain in patients with TMD. For sure this theme deserves not attention due to number of affected individuals, but more deep studies to understand its relationship with malocclusion and treatment possibilities.
Well, despite the fact that the patient or the tutors have to be notified of the facial asymmetry that persists, functional limitations will be presented. In more than 30 years of clinical experience treating these patients it was never sought the 4 first permanent molars and the 4 canines in the same Angle’s Class. In one side can be seen Class 1, but on the other it will be finding class 2 or class 3, the case reported exemplifies it, and the worst, mastication guidance will have to be very carefully done since, in most cases if it is tried to adjust the inferior and superior dental midline the vertical asymmetry of the occlusal plane (minimum vertical dimension) will worsen.
According to Planas [5] growth and development laws the mastication has to be made on the right side to stimulate mandibular length growth on the left side to correct the deviation. But according to Planas [5] growth and development laws to balance the occlusal plane avoiding that one side stays closer to Camper Plane than the other side the mastication has to be done on the left side. A real catch 22, what to do? Which is the less harmful limitation to the patient? What to do with the affected body posture of the patient? What are the body postural compensations. These questions deserve and must be investigated quickly to develop the best treatment protocol to these individuals.
4. Conclusions
Based on the case reported, non-treated plagiocephaly can bring serious limitations to malocclusion treatment results
Further studies are necessary to a better understanding of the situation plagiocephaly versus malocclusion.
References
-
J. Persing, H. James, J. Swanson, and J. Kattwinkel, “Prevention and management of positional skull deformities in infants,” Pediatrics, Vol. 112, No. 1, pp. 199–202, 2003.
-
B. K. Jung and I. S. Yun, “Diagnosis and treatment of positional plagiocephaly,” (in Spanish), Archives of Craniofacial Surgery, Vol. 21, No. 2, pp. 80–86, Apr. 2020, https://doi.org/10.7181/acfs.2020.00059
-
J. Ellwood, J. Draper-Rodi, and D. Carnes, “The effectiveness and safety of conservative interventions for positional plagiocephaly and congenital muscular torticollis: a synthesis of systematic reviews and guidance,” Chiropractic and Manual Therapies, Vol. 28, No. 1, pp. 1–11, Jun. 2020, https://doi.org/10.1186/s12998-020-00321-w
-
R. L. Morales Gaibor, “Plagiocefalia y sus efectos en la maloclusión dental,” (in Spanish), Jun. 2022.
-
P. Planas, Reabilitação Neuro-Oclusal. (in Portuguese), Médica e Científica, 1997.
-
W. A. Simões, Ortopedia Funzionale Dei Mascellari Attraverso La Riabilitazione Neuro-Occlusale. (in Italian), Trestina, Nike Srl, 2010.
-
O. Santiago Jr. and I. P. M. Santiago, Atlas De Construção De Aparelhos Ortopédicos Funcionais. (in Portuguese), Ribeirão Preto.
About this article

The authors have not disclosed any funding.
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ana Luiza Santos Felix: conceptualization, writing - original draft preparation. Sabrina Stefani Soares: conceptualization, writing-original draft preparation. Viviane Ferreira Lima: conceptualization, writing-original draft preparation. Orlando Santiago Junior: methodology, writing - original draft and reviewing, visualization.
The authors declare that they have no conflict of interest.
This study does not require epic committee approval since it is a retrospective case report, and the patient seeks spontaneously for treatment.
