Abstract
Nasal breathing plays a fundamental role in the functional balance of the Stomatognathic System and in the harmonious development of craniofacial structures. However, obstruction of the upper airways can lead to the establishment of predominantly oral breathing, a condition frequently associated with functional and morphological alterations during childhood. The aim of this study was to conduct a narrative literature review on the repercussions of mouth breathing on craniofacial growth in children. Studies addressing the etiology of mouth breathing, its craniofacial and functional repercussions, diagnostic methods, and therapeutic possibilities were analyzed. The literature shows that mouth breathing is associated with alterations in the facial growth pattern, including increased facial height, maxillary atresia, lip incompetence, mandibular retrognathism, open and crossed bites, as well as narrowing of the upper airways. Functional impairments related to chewing, swallowing, speech, sleep quality, school performance, and cognitive development were also observed. Early diagnosis and interdisciplinary intervention are shown to be essential for preventing or minimizing the repercussions of mouth breathing on children’s growth and development. It is concluded that mouth breathing can exert a significant influence on the craniofacial and functional development of children, reinforcing the importance of early identification and intervention.
Highlights
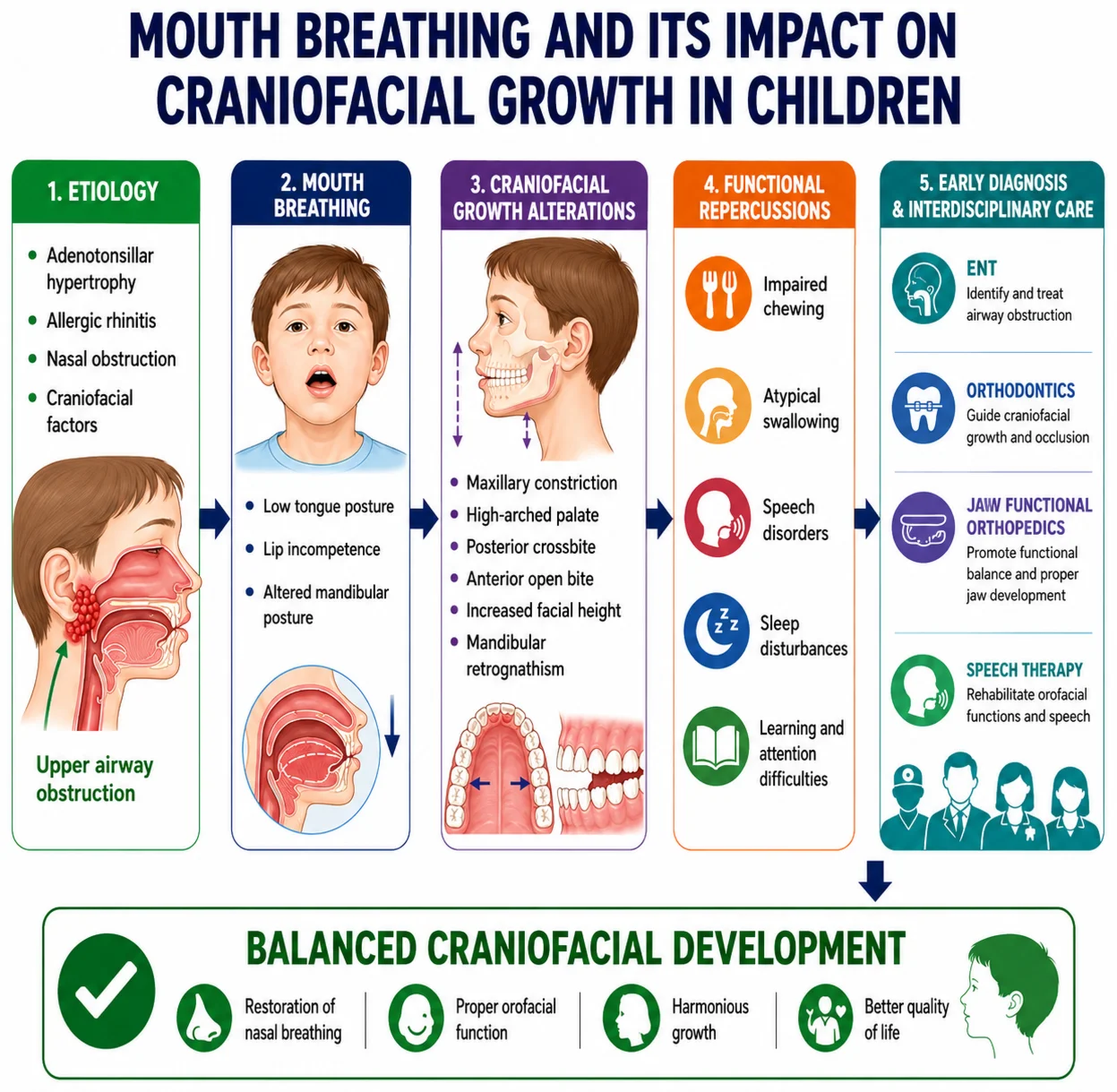
- Mouth breathing is associated with significant craniofacial alterations, including maxillary constriction, increased facial height, and mandibular retrognathism.
- Upper airway obstruction is a major etiological factor for mouth breathing and may influence craniofacial growth during childhood.
- Mouth breathing affects stomatognathic functions, contributing to atypical swallowing, speech disorders, and impaired chewing.
- Functional and morphological consequences of mouth breathing may negatively impact sleep quality, learning, attention, and overall child development.
- Early diagnosis and interdisciplinary management are essential to restore nasal breathing and promote balanced craniofacial development.
1. Introduction
Breathing is a vital, involuntary, and continuous function, indispensable for the maintenance of life. Under physiological conditions, pulmonary ventilation occurs predominantly through the nasal route, allowing inspired air to be filtered, warmed, and humidified before reaching the lungs. In addition to its importance for gas exchange, nasal breathing plays a fundamental role in the functional balance of the stomatognathic system and in the harmonious development of craniofacial structures [1, 2].
The maintenance of an adequate nasal breathing pattern is associated with correct lip and tongue posture, promoting balance among orofacial muscular forces. The interaction between nasal airflow and the position of the tongue against the palate contributes to adequate transverse and vertical growth of the jaws, favoring the balanced development of the craniofacial complex [2]. In this context, several authors emphasize that nasal costodiaphragmatic breathing is essential for the normal development of orofacial functions and the craniofacial skeleton, corroborating the principles of Moss's Functional Matrix Hypothesis [1].
However, when the patency of the upper airways is compromised, nasal breathing may be replaced by an oral or mixed breathing pattern. This condition may be related to mechanical, functional, or neurological factors and frequently results in alterations in muscular balance, stomatognathic system function, and occlusal development [3].
Mouth breathing has been associated with several systemic and craniofacial repercussions, including alterations in orofacial muscle function, postural deformities, malocclusions, and changes in facial growth. Studies show that this breathing pattern can negatively influence the structural development of the craniofacial region, reducing intraoral space and pharyngeal airway space, which can further compromise respiratory function and normal facial development [4].
Given the relevance of nasal breathing for craniofacial growth and the potential repercussions associated with mouth breathing, it becomes important to understand the mechanisms involved in this condition and its impacts during childhood. Thus, the present study aims to conduct a narrative literature review on the repercussions of mouth breathing on craniofacial growth in children.
2. Methodology
The present study consists of a narrative literature review, carried out with the aim of gathering and discussing scientific evidence on the repercussions of mouth breathing on craniofacial growth in children. For the development of this work, scientific publications available in the PubMed, Scielo, and Google Scholar databases were consulted, including original articles, literature reviews, systematic reviews, meta-analyses, and reference books related to the topic.
The bibliographic search was conducted using combinations of descriptors in Portuguese and English, such as: “Orthodontics”, “Malocclusion”, “Pediatric dentistry”, “Odontopediatria”, “Dentistry”, “Ortopedia Funcional dos Maxilares”, “Jaw Functional Orthopedics”, “Respiration”, “Respiração Nasal”, “Vias aéreas superiores”. Priority was given to studies published in recent years, without excluding classic works considered relevant to understanding the etiological, functional, and morphological aspects associated with mouth breathing.
After reading the titles, abstracts, and full texts, publications presenting information related to the etiology of mouth breathing, its craniofacial and functional repercussions, diagnostic methods, and therapeutic approaches were selected. The data obtained were analyzed descriptively and organized into thematic topics to support the discussion presented in this study.
3. Literature review
3.1. Etiology of mouth breathing
Mouth breathing can result from obstruction at any site along the upper airways [5]. Anatomical and functional factors influence respiratory obstruction. Anatomical factors include certain craniofacial deformities, the position of the hyoid bone, enlargement of the soft palate, adenotonsillar hypertrophy, and macroglossia. Functional factors include pharyngeal hypotonia caused by REM sleep and abnormal neurological control, among others [6].
Hyoid bone position: The hyoid bone and its associated muscles play an important role in maintaining upper airway patency. Studies suggest that obstructive respiratory alterations are frequently related to a more inferior and posterior positioning of this structure. Furthermore, the anatomical relationship between the hyoid bone, the mandible, and the cervical vertebrae remains relatively stable from three years of age onward, a period during which the hyoid, under normal conditions, is positioned at the level of the lower portion of the third cervical vertebra [7].
Skeletal factors: Craniofacial alterations, such as transverse maxillary deficiency and the presence of mandibular micrognathism or retrognathism, are considered anatomical factors capable of influencing upper airway patency and favoring the development of respiratory obstructions [8].
Soft tissues: Alterations in the soft tissues adjacent to the upper airways have also been associated with respiratory obstruction. Among the main changes observed are hypertrophy of the peripharyngeal structures, accumulation of cervical adipose tissue, fatty infiltration, and edema of the soft palate. These conditions can increase negative inspiratory pressure, favoring a more inferior positioning of the hyoid bone. Additionally, increased soft palate dimensions have been pointed out as a possible contributing factor to airway narrowing and the development of respiratory obstructions [7].
Inflammatory factor: Adenotonsillar hypertrophy is considered the main cause of upper airway obstruction and mouth breathing in childhood. The adenoids, located in the nasopharynx, and the palatine tonsils, located in the oropharynx, make up Waldeyer's lymphatic ring and may physiologically increase in size during childhood. However, when pathological hypertrophy occurs, these structures reduce the cross-sectional area of the pharynx, hindering nasal breathing and leading the child to breathe partially or entirely through the mouth. Nevertheless, the significance of infections and adenotonsillar hypertrophy is not limited to airway obstruction, as they can also affect adjacent structures, such as the nasal cavity, paranasal sinuses, and middle ear [5, 9].
In addition to adenotonsillar hypertrophy, other conditions capable of compromising nasal patency can also trigger mouth breathing. These include allergic rhinitis, chronic rhinitis, and sinusitis, the prevalence of which has increased in recent decades due to environmental degradation and air pollution. Anatomical alterations, such as nasal septum deviation, turbinate hypertrophy, nasal polyps, and sequelae of nasal trauma, can also reduce nasal airflow and favor the establishment of this breathing pattern [5].
Lingual factor: Macroglossia has been identified as a factor that may favor the occurrence of respiratory obstructions. In this context, several studies have evaluated the impact of orthodontic, orthopedic, and surgical treatments on the space available for tongue accommodation. Interventions such as maxillary expansion and the use of facial masks tend to increase intraoral volume, providing better conditions for tongue positioning. Conversely, some orthodontic treatments may reduce this space, altering tongue position and its relationship with the upper airways. Jaw Functional Orthopedics, in turn, seeks to promote a more physiological tongue position, as well as to expand its functional space within the oral cavity [8].
3.2. Craniofacial repercussions
Mouth breathing can cause significant alterations in craniofacial growth and development, especially when established during childhood, a period of intense functional and structural plasticity. According to Planas, once pathological neural circuits resulting from mouth breathing become established, it becomes difficult to restore previously existing physiological patterns. Furthermore, reduced nasal function can compromise the development of the nasal cavities and, consequently, the maxillary structures, since the palate forms the floor of the nasal cavity [10].
Maintaining an oral breathing pattern, whether during the day or during sleep, is associated with changes in the posture of the lips, tongue, and mandible, which directly affect craniofacial morphology. Among the alterations frequently observed are a low tongue position, lip incompetence, narrowing of the nasal base, maxillary compression, increased facial height, and an increased mandibular angle. However, the magnitude of these alterations depends on factors such as the intensity, duration, and timing of onset of the respiratory dysfunction [11].
Low tongue posture constitutes one of the main mechanisms involved in these alterations. Several authors report that maxillary atresia reduces the space available for adequate tongue accommodation, preventing its physiological positioning against the palate. As a consequence, the tongue assumes a lower position within the oral cavity, favoring maxillary compression and the development of posterior crossbite. In addition, this posture is associated with a reduction in oropharyngeal airway space. In this context, in 1984, observed a strong association between increased nasal resistance, decreased upper airway caliber, maxillary atresia, and mouth breathing, characteristics frequently found in individuals with obstructive sleep apnea syndrome [11].
The dentofacial repercussions of mouth breathing are widely described in the literature. Cuccia, Lotti, and Caradonna [12] observed that mouth-breathing children frequently present lip incompetence at rest, reduced transverse maxillary dimension, maxillary dental crowding, and adenoid facies. The authors also reported the presence of a narrow maxillary arch, deep palate, posterior crossbite, anterior open bite, and Class II or III malocclusions. In addition to dentoskeletal alterations, they identified characteristic postural adaptations, including reduced cervical lordosis and increased atlanto-occipital extension as a compensatory mechanism to facilitate airflow.
Similarly, Chambi-Rocha, Cabrera-Domínguez, and Domínguez-Reyes [13] demonstrated that mouth-breathing children present reduced anteroposterior dimensions of the upper airways compared to nasal breathers. In adolescents, the authors also observed additional alterations, such as a more elongated palate and a more inferior position of the hyoid bone in relation to the mandibular plane.
More recent studies reinforce this association between mouth breathing and alterations in the facial growth pattern. Topkal et al. [14] identified increased facial height, adenoid facial pattern, and mandibular retrognathism in mouth-breathing individuals. Similarly, Feștilă et al. [15] reported the frequent presence of adenoid facies, convex facial profile, increased lower facial height, lip incompetence, mandibular retrognathism, narrow maxilla, anterior open bite, maxillary dental crowding, and distalized occlusion.
Occlusal alterations are also closely related to mouth breathing. Grippaudo et al. [16] found a strong association between this breathing pattern and different types of malocclusion, including sagittal alterations, anterior and posterior crossbites, and open bites. Corroborating these findings, Festa et al. [17] suggested that malocclusion may play a bidirectional role in mouth breathing: in cases of mild upper airway obstruction, it may contribute to the establishment of oral breathing, whereas in cases of severe obstruction, it tends to arise as a consequence of the functional and structural adaptations resulting from respiratory difficulty.
Finally, Zhao et al. [4], in a systematic review with meta-analysis, observed that mouth-breathing children present a greater tendency toward vestibular inclination of the maxillary incisors and a higher frequency of upper airway narrowing. These findings reinforce the influence of mouth breathing on craniofacial growth and the development of malocclusions, highlighting the importance of early diagnosis and intervention to minimize its functional and morphological repercussions.
3.3. Functional repercussions
Mouth breathing is associated with several functional repercussions that can compromise a child's development and quality of life. In addition to alterations in craniofacial growth, this breathing pattern has been related to impairments in nutrition, body posture, sleep quality, school performance, and stomatognathic functions, particularly chewing, swallowing, and speech [18]. The alterations in posture, tone, and mobility of the lips, tongue, and cheeks frequently observed in mouth breathers can reduce the efficiency of stomatognathic functions. In addition, structural changes such as maxillary atresia and malocclusions contribute to functional impairment of the stomatognathic system [18, 19].
Swallowing is one of the functions most frequently affected in these individuals. Evidence shows that patients with mouth breathing present a higher risk of developing atypical swallowing, a condition also associated with tonsillar and adenoid hypertrophy. Since breathing and swallowing are closely coordinated functions, the absence of adequate lip seal favors tongue interposition during swallowing as a compensatory mechanism to achieve the necessary seal. Thus, the high incidence of atypical swallowing in mouth breathers reinforces the close relationship between respiratory alterations and orofacial myofunctional disorders [20].
Speech can also be significantly influenced by mouth breathing. Adequate speech sound production depends on the integrity of the orofacial structures, as well as the correct positioning and mobility of the phonoarticulatory organs. Alterations in the posture, tone, and mobility of the tongue, lips, and cheeks, associated with structural changes resulting from alterations in craniofacial growth and occlusion, can compromise phoneme articulation [19]. Among the speech disorders most frequently described in mouth breathers are anterior tongue positioning during the production of dental phonemes, anterior and lateral lisping (sigmatism), and difficulties in articulating bilabial and fricative sounds [18, 22]. These alterations can impair speech intelligibility and negatively affect a child's communication, social relationships, and emotional well-being [22].
In addition to myofunctional repercussions, the literature reports that mouth-breathing children present a greater predisposition to attention deficits, impairments in working memory, reading difficulties, alterations in mathematical performance, and other learning disorders [21]. Such alterations may be related to daytime sleepiness, reduced cerebral oxygenation, and changes in auditory processing. Additionally, the greater susceptibility to ear infections resulting from adenotonsillar hypertrophy and alterations in the auditory tube can result in fluctuating hearing loss, interfering with the perception of speech sounds during important periods of child development and contributing to delays and alterations in language [18].
3.4. Clinical and imaging diagnosis
The clinical diagnosis of mouth breathing is based on identifying characteristic signs and symptoms observed during history-taking and physical examination. Among the main clinical findings are lip incompetence, dry lips, low tongue posture, high-arched palate, maxillary atresia, occlusal alterations, audible breathing, and typical facial characteristics such as a long, narrow face. Postural alterations may also be present, including forward head posture, spinal alterations, and impaired pulmonary ventilation. During history-taking, a history of recurrent respiratory infections, sinusitis, tonsillitis, otitis, and sleep disorders is common. Furthermore, many patients present behavioral and psychosocial repercussions, such as irritability, daytime sleepiness, attention deficit, learning difficulties, and alterations in language development [23].
Imaging evaluation plays an important role in the diagnosis of upper airway alterations associated with mouth breathing. Among the available methods, cone-beam computed tomography (CBCT) has been widely used in different healthcare areas, including otorhinolaryngology, for investigating alterations in the paranasal sinuses, nasal cavity, nasopharynx, and other structures related to upper airway patency. With technological advances, CBCT has come to be widely used in the evaluation of adenoid hypertrophy, allowing not only the identification of this condition but also contributing to treatment planning and clinical follow-up [24]. When compared to conventional medical computed tomography, CBCT presents lower cost and reduced radiation exposure. However, its radiographic dose remains higher than that of the two-dimensional radiographic examinations traditionally used in clinical practice [25].
Lateral cephalometric radiography remains one of the most frequently used examinations in orthodontic evaluation and in the study of the upper airways. Although it is not considered the gold standard for diagnosing respiratory obstructions, it constitutes a useful method due to its low cost, ease of execution, standardization, and wide availability. Furthermore, it is a non-invasive, easily interpreted examination that requires little patient cooperation during its performance [8]. Feng et al. [25] suggested that cephalometric measurements obtained from this examination, such as the AN ratio, can be used as a screening method to estimate nasopharyngeal volume.
However, the main limitation of lateral cephalometric radiography lies in the fact that it provides only a two-dimensional representation of three-dimensional anatomical structures. As a result, alterations located in the transverse plane may not be adequately identified, reducing diagnostic accuracy in certain situations [6]. In contrast, three-dimensional examinations, such as computed tomography and magnetic resonance imaging, allow for a more detailed evaluation of upper airway morphology and dimensions, enabling more precise quantitative and qualitative analyses, including measurement of their transverse diameters [8].
Through cephalometric analysis it is possible to evaluate: craniofacial and upper airway anatomical alterations that may contribute to the development of certain respiratory conditions, such as Obstructive Sleep Apnea Syndrome (OSAS); changes in hyoid bone position and postural adaptations of the cervical spine, which may interfere with head positioning at rest; the characteristics of the upper airways, allowing analysis of the nasopharyngeal, oropharyngeal, and hypopharyngeal regions; the alterations resulting from different therapeutic approaches, including rapid maxillary expansion, mandibular advancement appliances, and Jaw Functional Orthopedic devices; and the relationship between skeletal structures and soft tissues in individuals with sleep-related breathing disorders [26].
Among the most widely used methods for cephalometric evaluation of the upper airways is the airway analysis proposed by McNamara (1984), developed from cephalometric concepts previously described by Ricketts and Harvold. This analysis is based on measuring the upper and lower pharyngeal spaces, allowing evaluation of upper airway patency and identification of possible reductions in caliber. In general, decreased values of these measurements are associated with airway space narrowing and reduced respiratory patency, while increased values indicate wider airways [27].
In addition to McNamara's analysis, the cephalometric protocol developed by the Federal University of São Paulo (UNIFESP), within the discipline of Sleep Medicine and Biology, has been widely used in the investigation of sleep-related breathing disorders. This method brings together, in a single analysis, different cephalometric variables related to craniofacial morphology and the upper airways, allowing a more comprehensive evaluation of the anatomical factors involved in respiratory alterations. The UNIFESP analysis encompasses six main dimensions: anteroposterior pattern, vertical pattern, cranial base, soft palate, pharyngeal airway space, and hyoid bone position. The anteroposterior and vertical dimensions allow evaluation of the position of the maxilla and mandible in relation to the cranial base and the facial growth pattern. The soft palate analysis provides important information about its morphology, while evaluation of the pharyngeal airway space allows investigation of the upper and lower regions of the pharynx, frequently related to obstructive sleep-related breathing disorders [11].
Another relevant aspect of this protocol is the evaluation of hyoid bone position, a structure closely related to the tongue, mandible, and upper airway patency. Analysis of its vertical and anteroposterior positions allows the identification of possible anatomical adaptations associated with respiratory alterations. Thus, the combination of McNamara's and UNIFESP's analyses provides important information on craniofacial morphology, pharyngeal airway space, and the anatomical factors potentially related to mouth breathing and sleep-related breathing disorders [11, 27].
3.5. Interdisciplinary management
Mouth breathing is a condition of multifactorial etiology that can compromise different aspects of child growth and development, requiring a multidisciplinary approach for both diagnosis and treatment. Its influence on the relationship between form, posture, and function of the craniofacial complex means that respiratory alterations can affect not only the upper airways but also facial growth, dental occlusion, and stomatognathic functions. In this context, early diagnosis is essential, as it enables the implementation of preventive and interceptive measures capable of minimizing or avoiding the development of more severe structural and functional alterations [28].
Due to the complexity of this condition, the management of mouth breathers should involve different healthcare professionals, including pediatricians, allergists, otorhinolaryngologists, orthodontists, jaw functional orthopedists, speech-language pathologists, and physical therapists. The otorhinolaryngologist is responsible for the diagnosis and treatment of upper airway obstructions, while the speech-language pathologist works on the rehabilitation of orofacial functions after removal of the obstructive cause. The orthodontist and/or jaw functional orthopedist, in turn, plays a fundamental role in the prevention and correction of craniofacial growth alterations. Thus, integration among the different specialties is essential to restore nasal breathing and promote the patient's adequate development [23].
This approach is justified by the fact that the impairments associated with mouth breathing go beyond craniofacial alterations. According to Marchi et al. [28], mouth-breathing individuals may present impairments of various kinds, including facial bone deformities, cardiorespiratory and immunological alterations, behavioral and cognitive changes, and difficulties with socialization. Corroborating these findings, Alhazmi [22], highlights the importance of multidisciplinary follow-up for mouth-breathing children, emphasizing that early identification and treatment are essential to prevent the adverse effects of this condition and to promote the individuals’ adequate physical, functional, and psychosocial development.
4. Discussion
The literature analyzed demonstrates that mouth breathing is associated with several craniofacial and functional alterations that can compromise child development. The studies reviewed indicate that upper airway obstruction favors the establishment of an oral breathing pattern, triggering muscular and postural adaptations capable of influencing craniofacial growth. Regarding morphological alterations, the studies reviewed showed that mouth breathing is associated with different craniofacial changes. Among these are increased facial height, maxillary narrowing, lip incompetence, mandibular retrognathism, and malocclusions, although not all of these were observed by every author. Taken together, the findings suggest that the oral breathing pattern can influence craniofacial development in children [12-15].
In addition to skeletal and dental alterations, several authors highlighted reduced upper airway dimensions in mouth-breathing individuals. Chambi-Rocha et al. [13] observed decreased anteroposterior airway dimensions, while Zhao et al. [4] found a higher frequency of upper airway narrowing in mouth-breathing children. These results suggest a close relationship between respiratory alterations and the craniofacial changes observed in these patients [4, 13].
The studies also showed an association between mouth breathing and different types of malocclusion. Grippaudo et al. [16] found a relationship between this breathing pattern and open bites, crossbites, and sagittal alterations. Similarly, Festa et al. [17] highlighted the existence of a relationship between upper airway obstruction, mouth breathing, and the development of malocclusions [16, 17].
At the functional level, the literature shows that mouth breathing can compromise important functions of the stomatognathic system. Gómez-González et al. [20] observed a higher occurrence of atypical swallowing in mouth breathers, while Hitos et al. [18], Nishimura and Gimenez [19], and Alhazmi [22] reported speech-related alterations. Furthermore, Warnier et al. [21] described an association between mouth breathing, attention deficit, learning difficulties, and cognitive impairments, demonstrating that its repercussions extend beyond craniofacial alterations.
Given these findings, the importance of early diagnosis and interdisciplinary management of mouth breathing becomes evident. As highlighted by Ianni Filho et al. [23], Marchi et al. [28], and Alhazmi [22], integration among different healthcare professionals is essential to identify etiological factors, restore nasal breathing, and minimize the functional and craniofacial repercussions associated with this condition [22, 23, 28].
5. Conclusions
Mouth breathing constitutes a multifactorial condition capable of significantly influencing craniofacial growth and development in children. The literature reviewed demonstrates that this breathing pattern is associated with morphological and functional alterations, including changes in facial growth, maxillary narrowing, malocclusions, postural alterations, and impairment of stomatognathic functions such as chewing, swallowing, and speech. Furthermore, repercussions on sleep quality, school performance, and the child's overall development may also occur.
Given these findings, the importance of early diagnosis and identification of the etiological factors involved is highlighted, enabling timely interventions capable of minimizing or preventing more severe alterations. In this context, interdisciplinary collaboration among different healthcare professionals is essential for restoring nasal breathing and promoting adequate craniofacial growth and development in children.
References
-
J. Barrientos, “Attention deficit and mouth breathing in children treated with functional maxillary orthopedics VI region 2012-2013,” (in Spanish), Porto Seguro, Study of prevalence, 2013.
-
S. Rodríguez, J. Smith-Ágreda, and N. García, Anatomy of the Organs of Language, Vision and Hearing. (in Spanish), Madrid: Editorial Médica Panamericana, 2003.
-
A. S. M. Pereira, M. Gatti, V. V. Ribeiro, K. V. M. Taveira, and G. Berretin-Felix, “Speech language pathology interventions in the areas of breathing, chewing, swallowing and speaking: a scoping review,” CoDAS, Vol. 36, No. 2, p. 20220339, Jan. 2024, https://doi.org/10.1590/2317-1782/20232022339en
-
Z. Zhao, L. Zheng, X. Huang, C. Li, J. Liu, and Y. Hu, “Effects of mouth breathing on facial skeletal development in children: a systematic review and meta-analysis,” BMC Oral Health, Vol. 21, No. 1, p. 108, Mar. 2021, https://doi.org/10.1186/s12903-021-01458-7
-
L. Lin, T. Zhao, D. Qin, F. Hua, and H. He, “The impact of mouth breathing on dentofacial development: a concise review,” Frontiers in Public Health, Vol. 10, p. 929165, Sep. 2022, https://doi.org/10.3389/fpubh.2022.929165
-
M. Riera, “Upper airway changes in adult patients treated with orthodontic extraction of four premolars,” University of Oviedo, 2014.
-
C. Johnston and Richardson, “Cephalometric changes in adult pharyngeal morphology,” The European Journal of Orthodontics, Vol. 21, No. 4, pp. 357–362, 1999, https://doi.org/10.1093/ejo/21.4.357
-
C. Barreiro, “Changes in the upper airway with orthopedic treatment of Class III,” (in Spanish), University of Oviedo, 2014.
-
Z. Abramson, S. Susarla, M. Troulis, and L. Kaban, “Age-related changes of the upper airway assessed by 3-dimensional computed tomography,” Journal of Craniofacial Surgery, Vol. 20, No. Suppl 1, pp. 657–663, 2009, https://doi.org/10.1097/scs.0b013e318193d521
-
P. Planas, Neuro-occlusal rehabilitation. Spain: Amolca, 2008.
-
C. Dal Fabbro, C. Chaves Junior, and S. Tufik, Dentistry in Sleep Medicine. (in Portuguese), Maringá: Dental Press, 2012.
-
A. M. Cuccia, M. Lotti, and D. Caradonna, “Oral breathing and head posture,” The Angle Orthodontist, Vol. 78, No. 1, pp. 77–82, Jan. 2008, https://doi.org/10.2319/011507-18.1
-
A. Chambi-Rocha, M. E. Cabrera-Domínguez, and A. Domínguez-Reyes, “Breathing mode influence on craniofacial development and head posture,” Jornal De Pediatria, Vol. 94, No. 2, pp. 123–130, Mar. 2018, https://doi.org/10.1016/j.jped.2017.05.007
-
K. G. Topsakal, E. Yurdakurban, G. S. Duran, and S. Görgülü, “3D evaluation of cranial and dentofacial morphological differences between individuals with mouth breathing and nasal breathing,” Journal of Stomatology, Oral and Maxillofacial Surgery, Vol. 125, No. 5, p. 101854, Oct. 2024, https://doi.org/10.1016/j.jormas.2024.101854
-
D. Feștilă, C. D. Ciobotaru, T. Suciu, C. D. Olteanu, and M. Ghergie, “Oral breathing effects on malocclusions and mandibular posture: complex consequences on dentofacial development in pediatric orthodontics,” Children, Vol. 12, No. 1, p. 72, Jan. 2025, https://doi.org/10.3390/children12010072
-
C. Grippaudo et al., “Association between oral habits, mouth breathing and malocclusion,” Acta Otorhinolaryngologica Italica: Organo Ufficiale Della Societa Italiana Di Otorinolaringologia E Chirurgia Cervico-facciale, Vol. 36, No. 5, pp. 386–389, 2016.
-
P. Festa et al., “Association between upper airway obstruction and malocclusion in mouth-breathing children,” Acta Otorhinolaryngologica Italica, Vol. 41, No. 5, pp. 436–442, 2021, https://doi.org/10.14639/0392-100x-n1225
-
S. F. Hitos, R. Arakaki, D. Solé, and L. L. M. Weckx, “Oral breathing and speech disorders in children,” Jornal De Pediatria, Vol. 89, No. 4, pp. 361–365, Jul. 2013, https://doi.org/10.1016/j.jped.2012.12.007
-
C. M. Nishimura and S. R. M. L. Gimenez, “Speech profile of the mouth breather,” Revista CEFAC, Vol. 12, No. 3, pp. 505–508, 2010, https://doi.org/10.1590/s1516-18462010005000044
-
C. Gómez-González, A. González-Mosquera, M. H. Alkhraisat, and E. Anitua, “Mouth breathing and its impact on atypical swallowing: a systematic review and meta-analysis,” Dentistry Journal, Vol. 12, No. 2, p. 21, Jan. 2024, https://doi.org/10.3390/dj12020021
-
M. Warnier, L. Piron, D. Morsomme, and C. Maillart, “Assessment of mouth breathing by speech-language pathologists: an international Delphi consensus,” CoDAS, Vol. 35, No. 3, Jan. 2023, https://doi.org/10.1590/2317-1782/20232022065
-
W. A. Alhazmi, “Mouth breathing and speech disorders: a multidisciplinary evaluation based on the etiology,” Journal of Pharmacy and Bioallied Sciences, Vol. 14, No. Suppl 1, pp. S911–S916, Jul. 2022, https://doi.org/10.4103/jpbs.jpbs_235_22
-
D. Ianni Filho et al., “Multidisciplinary contribution to the diagnosis and treatment of nasopharyngeal obstructions and mouth breathing,” (in Portuguese), Revista Clínica de Ortodontia Dental Press, Vol. 4, No. 6, pp. 90–102, 2006.
-
Y. Wang et al., “Significance of nasopharyngeal cavity area in individuals with adenoid hypertrophy assessed by cone beam computed tomography,” Ear, Nose and Throat Journal, 2023, https://doi.org/10.1177/01455613231212837
-
X. Feng, Y. Chen, W. Cai, S. A. Lie, K. Hellén-Halme, and X.-Q. Shi, “Aerodynamic characteristics in upper airways among orthodontic patients and its association with adenoid nasopharyngeal ratios in lateral cephalograms,” BMC Medical Imaging, Vol. 21, No. 1, p. 127, Aug. 2021, https://doi.org/10.1186/s12880-021-00659-4
-
C. Villafranca, J. Cobo-Plana, M. Fernández-Mondragón, and A. Jiménez, “Cephalometry of the upper airways,” (in Portuguese), RCOE, Vol. 7, No. 4, pp. 407–414, 2002.
-
J. Gregoret, Orthodontics and orthognathic surgery: diagnosis and planning. (in Spanish), Barcelona: Espaxs Publicaciones Médicas, 2003.
-
R. C. C. Marchi et al., “The need for multidisciplinarity in the treatment of mouth breathers,” Revista Científica Saúde E Tecnologia, Vol. 3, No. 6, 2023.
About this article

The authors have not disclosed any funding.
The author thanks the Federal University of Alfenas (UNIFAL-MG) for granting the teaching assistantship scholarship in the discipline of Preventive and Interceptive Orthodontics, whose support contributed to her academic education and to the development of the teaching and research activities that made this work possible.
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Marina Naves Pereira: conceptualization, data curation, investigation, methodology, literature review, writing-original draft preparation, writing-review and editing. Isadora Stella Souza e Andrade: investigation, writing-original draft preparation, writing-review and editing. Lorena Gomes Marchant: investigation, writing-original draft preparation, writing-review and editing. Irene Acevedo: investigation, writing-original draft preparation, writing-review and editing. Márcia do Amaral Sampaio: methodology, writing-original draft preparation, writing-review and editing. Luciano Aparecido de Almeida-Junior: supervision, conceptualization, data curation, investigation, methodology, literature review, writing-original draft preparation, writing-review and editing.
The authors declare that they have no conflict of interest.
Present study consists of a narrative literature review based exclusively on previously published scientific data available in public databases (PubMed, SciELO, and Google Scholar).
As this study does not involve the direct collection of data from human or animal subjects, does not include clinical interventions, does not use biological samples, and does not access personal or confidential information of any individuals, it is exempt from submission to and approval by a Research Ethics Committee (REC/IRB), in accordance with the applicable national and international ethical guidelines governing scientific research.
All sources consulted were properly cited, and no individual or unpublished data were used without appropriate authorization.
