Abstract
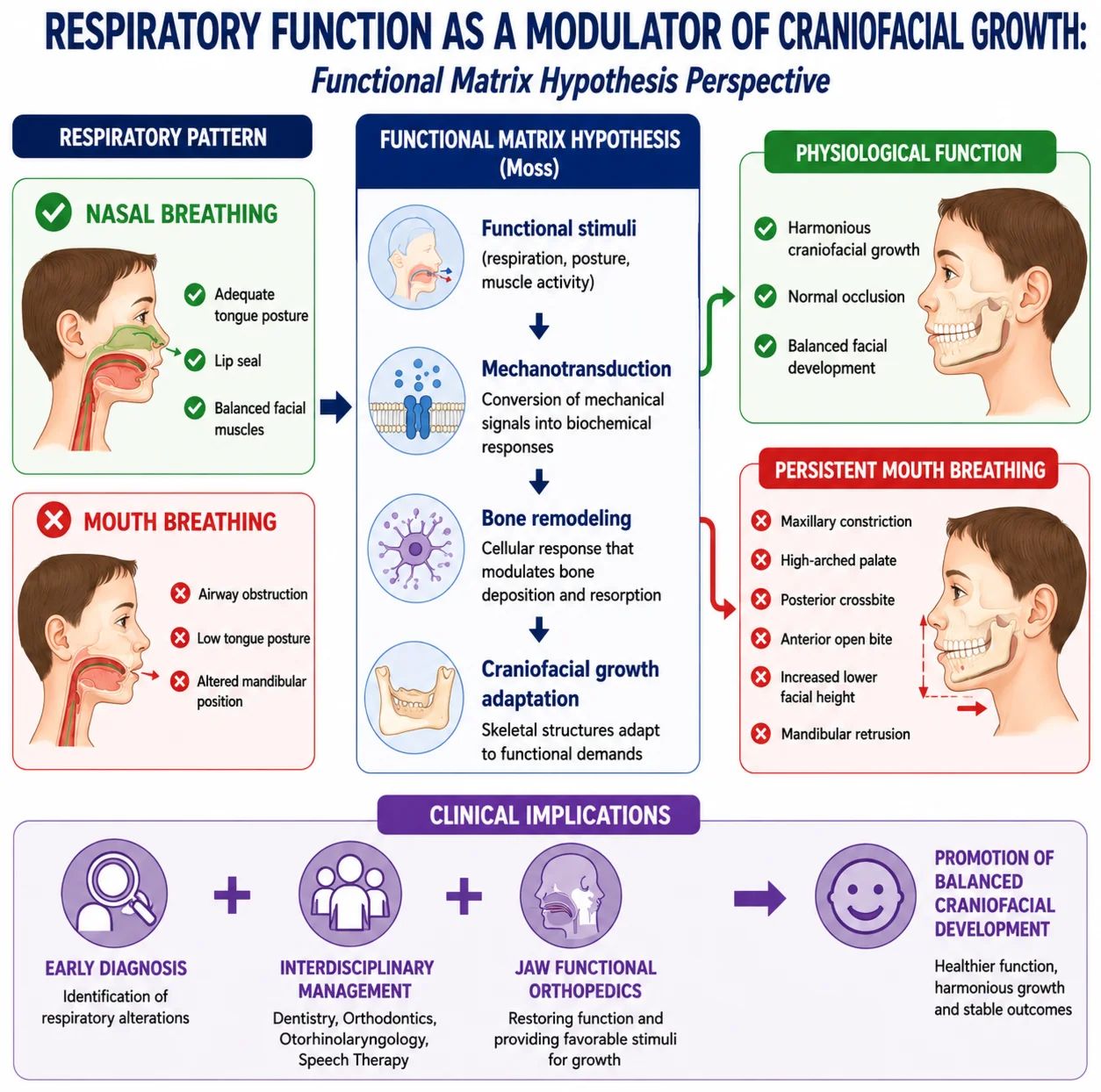
The craniofacial growth process results from the interaction among genetic, epigenetic, and environmental factors, with functional stimuli being fundamental to the development of the stomatognathic system. Among these stimuli, respiratory function exerts significant influence on craniofacial morphology and the establishment of normal occlusion. Functional alterations, especially chronic mouth breathing, can modify muscular balance, tongue posture, mandibular positioning, and facial growth patterns, contributing to the development of dentofacial anomalies and malocclusions. In this context, the Functional Matrix Hypothesis, proposed by Moss, provides a theoretical framework for understanding how functional demands influence craniofacial growth and remodeling. The present study aimed to analyze the influence of respiratory function on craniofacial growth from the perspective of the Functional Matrix Hypothesis, through a narrative literature review. A qualitative and descriptive review was conducted using scientific publications indexed in the PubMed, SciELO, and Google Scholar databases, including both classical and contemporary studies related to craniofacial growth, respiratory function, mouth breathing, mechanotransduction, and the Functional Matrix Hypothesis. The results indicate that nasal breathing contributes to harmonious craniofacial development, whereas persistent mouth breathing may lead to structural and functional adaptations associated with maxillary atresia, increased lower facial third height, posterior crossbite, open bite, and mandibular retrusion. Furthermore, the evidence reviewed highlights the importance of early diagnosis and an interdisciplinary approach to respiratory dysfunctions. Jaw Functional Orthopedics stands out as an important therapeutic alternative by promoting favorable functional conditions for craniofacial growth and development. It is concluded that respiratory function acts as a significant modulator of craniofacial growth, reinforcing the relevance of preventive and interceptive strategies aimed at restoring physiological functions and promoting balanced craniofacial development.
Highlights
- Respiratory function is a significant modulator of craniofacial growth and development throughout childhood and adolescence.
- According to the Functional Matrix Hypothesis, functional stimuli influence craniofacial morphology through mechanotransduction and bone remodeling.
- Persistent mouth breathing is associated with maxillary constriction, increased facial height, mandibular retrusion, and malocclusions.
- Physiological nasal breathing promotes balanced stomatognathic function and harmonious craniofacial development.
- Early diagnosis and interdisciplinary management of respiratory dysfunctions may help prevent dentofacial alterations and improve growth outcomes.
1. Introduction
Craniofacial growth and development constitute complex biological processes resulting from the interaction among genetic, epigenetic, environmental, and functional factors. According to Moyers [1], growth corresponds to the quantitative increase of biological structures, while development encompasses the qualitative modifications responsible for the functional maturation of tissues and organs. In this context, the formation of the craniofacial complex occurs in a dynamic and continuous manner, being influenced by multiple factors acting simultaneously throughout growth [1, 2].
Recent advances in the understanding of the craniofacial complex have demonstrated that facial development does not depend exclusively on genetics, but also on the constant interaction between environmental factors and functional stimuli. Stimson and Jones [3] emphasize that craniofacial growth results from the integration of intrinsic biological mechanisms and external influences capable of modifying the trajectory of facial development. Likewise, Capote, Preston, and Kapadia [4] highlight that the functions performed by the Stomatognathic System (SS) play an important role in the modeling and remodeling of craniofacial structures during childhood and adolescence.
Among these functions, respiration is of particular relevance due to its influence on the posture of the tongue, lips, mandible, and perioral musculature. Physiological nasal breathing promotes the functional balance of the SS and contributes to the harmonious development of facial structures. In contrast, alterations in upper airway permeability may lead to the establishment of mouth breathing, triggering muscular and postural adaptations capable of influencing craniofacial growth [5, 6].
The association between mouth breathing and craniofacial alterations has been extensively investigated in the scientific literature. Recent evidence demonstrates that children with a mouth-breathing pattern show a greater tendency toward the development of maxillary narrowing, increased facial vertical dimension, deep palate, mandibular retrusion, and malocclusions, when compared to those with predominantly nasal breathing [7-9].
The understanding of this relationship finds important theoretical grounding in the Functional Matrix Hypothesis (FMH), proposed by Moss [10], according to which the growth of skeletal tissues occurs as a secondary response to the functional demands of soft tissues and their associated functional spaces. Subsequently, Moss [11] expanded this hypothesis by incorporating the mechanisms of mechanotransduction, reinforcing the influence of physiological functions on bone remodeling and craniofacial growth.
Given this context, it becomes relevant to understand how respiratory function can influence craniofacial development and in what way the principles of the FMH contribute to the interpretation of these alterations. Thus, the objective of this narrative review is to analyze the influence of respiratory function on craniofacial growth from the perspective of the Functional Matrix Hypothesis, discussing current scientific evidence and its clinical implications for the prevention and treatment of dentofacial alterations.
2. Methodology
The present study consists of a narrative literature review, conducted with the aim of gathering and discussing scientific evidence regarding the repercussions of Moss’s Functional Matrix Hypothesis in relation to respiration as an epigenetic stimulus. For the elaboration of this work, scientific publications available in the PubMed, SciELO, and Google Scholar databases were consulted, including original articles, literature reviews, systematic reviews, meta-analyses, and reference books related to the topic.
The bibliographic search was conducted using combinations of descriptors in Portuguese and English, such as: “Orthodontics”, “Malocclusion”, “Pediatric Dentistry”, “Dentistry”, “Hypothesis of the Functional Matrix”, and “Respiration”. Studies published in recent years were prioritized, without excluding classic works considered relevant to the understanding of the etiological, functional, and morphological aspects associated with oral breathing.
After reading titles, abstracts, and full texts, publications presenting information related to the etiology of oral breathing, its craniofacial and functional repercussions, diagnostic methods, and therapeutic approaches were selected. The data obtained were analyzed descriptively and organized into thematic topics to support the discussion presented in this study.
3. Literature review
3.1. Functional matrix hypothesis
The development of craniofacial structures occurs through the continuous interaction between biological and environmental factors, being influenced by the functions performed by the stomatognathic system throughout life – Moyers [18]. In a complementary manner, facial morphology results from continuous processes of bone remodeling that respond to the functional demands of the organism [12].
Among the theories that seek to explain the mechanisms of craniofacial growth, the Functional Matrix Hypothesis, proposed by Moss [10], stands out. This hypothesis establishes that skeletal tissues do not constitute the primary determinant of facial growth, but rather respond to the functional needs of soft tissues and their associated functional matrices. Thus, functional alterations would be capable of directly influencing craniofacial morphology during growth.
Subsequently, Moss [11] revisited his theory by incorporating concepts related to cellular mechanotransduction. According to this approach, mechanical stimuli generated by physiological functions are converted into biochemical signals capable of modulating cellular activity and bone remodeling. These concepts remain relevant to the contemporary understanding of the structural adaptation processes observed during craniofacial growth.
Respiration plays a fundamental role in maintaining the functional balance of the stomatognathic system. Physiological nasal breathing promotes the adequate positioning of the tongue against the palate, passive lip sealing, and the balance of facial musculature. When this pattern is altered, compensatory adaptations may occur, influencing the dynamics of facial growth [5].
Mouth breathing is frequently associated with the presence of upper airway obstructions, such as adenoid hypertrophy, tonsillar hypertrophy, and allergic rhinitis. These conditions can modify the posture of the tongue, mandible, and head, altering the distribution of functional forces on craniofacial structures [13, 8, 9].
Grippaudo et al. [6] observed a significant association between mouth breathing, deleterious oral habits, and a higher prevalence of malocclusions in children. The authors emphasize that persistent functional alterations during growth periods can compromise the adequate development of dentoskeletal structures.
Zhao et al. [7], in a systematic review and meta-analysis, demonstrated that mouth-breathing children show a greater tendency toward transverse maxillary narrowing, increased lower facial third, mandibular retrusion, and alterations in dental positioning. These results reinforce the hypothesis that respiratory function exerts a direct influence on craniofacial growth patterns.
In addition to morphological alterations, recent research has demonstrated the importance of orofacial myofunctional therapy in the rehabilitation of stomatognathic system functions. Villa et al. [15] found that myofunctional therapy can promote significant improvement in the respiratory pattern and muscular function in children with sleep-disordered breathing. Similarly, Liu et al. [14] observed that myofunctional intervention has the potential to positively contribute to the craniofacial development of children with respiratory alterations. More recently, Saba et al. [16], in a systematic review and meta-analysis, highlighted that orofacial myofunctional therapy may represent an important complementary strategy in the management of respiratory alterations, promoting functional improvement and contributing to the stability of therapeutic outcomes.
Thus, the current scientific literature supports that respiratory function represents an important modulating factor of craniofacial growth. From the perspective of the Functional Matrix Hypothesis, respiratory alterations can be understood as modifications of functional matrices capable of influencing the development of facial skeletal structures, reinforcing the importance of early diagnosis and an interdisciplinary approach for the prevention and treatment of dentofacial alterations.
3.2. Clinical implications in the prevention of malocclusions
Current scientific evidence reinforces that the early identification of respiratory alterations constitutes an important strategy for the prevention of malocclusions. Persistent functional alterations during critical growth periods may favor the development of posterior crossbite, anterior open bite, maxillary atresia, and skeletal discrepancies [6, 7].
In this scenario, the early clinical monitoring of children showing signs of mouth breathing should be integrated into preventive protocols in Pediatric Dentistry, Preventive and Interceptive Orthodontics, and craniofacial growth follow-up. Pacheco et al. [5] emphasize the importance of early clinical identification of altered respiratory patterns, enabling timely interventions and reduction of impacts on facial development.
The management of these alterations requires an interdisciplinary approach involving pediatric dentists, orthodontists, jaw functional orthopedists, otorhinolaryngologists, and speech-language Pathologists. The correction of etiological factors associated with upper airway obstruction, combined with functional rehabilitation, can contribute to the normalization of the respiratory pattern and the restoration of stimuli favorable to craniofacial growth [8, 9].
3.3. Role of jaw functional orthopedics
Jaw Functional Orthopedics presents itself as a therapeutic approach compatible with the principles of functional adaptation of craniofacial growth described by the FMH. From this perspective, treatment is not limited to the structural correction of dentoskeletal alterations, but seeks to promote functional conditions favorable to the balanced development of the stomatognathic system [17].
Recent studies demonstrate that orofacial myofunctional therapy can promote significant improvements in respiratory function, lingual posture, and perioral muscle activity, especially when implemented during the growth phase [15, 14]. Furthermore, recent systematic reviews indicate that functional rehabilitation can contribute to the stability of therapeutic outcomes and to the improvement of respiratory quality in children with sleep-disordered breathing [16].
Thus, early functional intervention, combined with adequate diagnosis of respiratory alterations, can contribute not only to the correction of existing alterations, but also to the prevention of future dentoskeletal discrepancies, reinforcing the importance of respiratory function as a modulating factor of craniofacial growth.
4. Discussion
The findings of the present review reinforce that respiratory function plays a relevant role in craniofacial growth and development, influencing the structural and functional organization of the craniofacial complex during the critical periods of childhood and adolescence. Although facial growth is determined by a complex interaction among genetic, epigenetic, and environmental factors, contemporary evidence demonstrates that functional stimuli exert significant influence on the expression of this biological potential [12, 3, 4].
The Functional Matrix Hypothesis proposed by Moss [10] and the subsequent expansion of the concept incorporating mechanotransduction [11] remain important theoretical frameworks for understanding the relationship between function and craniofacial growth. In this context, physiological nasal breathing promotes the functional balance of the SS through the adequate maintenance of lingual posture, lip sealing, and perioral muscle activity. In contrast, chronic mouth breathing can trigger neuromuscular adaptations capable of altering the facial growth pattern. Recent studies have demonstrated a consistent association between mouth breathing and skeletal alterations, such as transverse maxillary narrowing, increased lower facial third, posterior mandibular rotation, deep palate, and a higher prevalence of malocclusions [6, 7].
The results presented by Zhao et al. [7] demonstrate that mouth-breathing children exhibit significantly more frequent craniofacial alterations when compared to those with a nasal respiratory pattern. These findings corroborate the clinical observations described by Grippaudo et al. [6], who identified an association between mouth breathing, deleterious oral habits, and the development of malocclusions.
Furthermore, recent studies highlight that respiratory alterations are frequently associated with obstructive conditions of the upper airways, such as adenoid hypertrophy, tonsillar hypertrophy, and sleep-disordered breathing. These conditions promote compensatory postural adaptations involving the tongue, mandible, and facial musculature, contributing to progressive changes in craniofacial morphology [8, 9].
5. Conclusions
The present narrative review has shown that respiratory function exerts significant influence on craniofacial growth and development, acting as an important modulating factor of facial morphology during childhood and adolescence. The scientific evidence analyzed demonstrates that physiological nasal breathing promotes the functional balance of the stomatognathic system, while persistent mouth breathing is associated with structural alterations capable of compromising the harmonious development of the face [6, 7].
The results also demonstrate that the principles of the FMH remain relevant for understanding the mechanisms involved in craniofacial morphogenesis. Recent advances in the study of facial growth and respiratory function reinforce the idea that skeletal structures continuously respond to functional stimuli arising from soft tissues and the upper airways [10, 11, 4].
From a clinical standpoint, the findings highlight the importance of early identification of respiratory alterations and the implementation of therapeutic strategies aimed at restoring physiological nasal breathing. The interdisciplinary collaboration among dentistry, orthodontics, jaw functional orthopedics, otorhinolaryngology, and speech-language pathology proves essential for minimizing the impacts of respiratory dysfunctions on craniofacial growth and for promoting more stable outcomes throughout development [5, 8].
Therefore, it is concluded that respiratory function represents an important determinant of craniofacial growth and should be considered an essential component in the clinical evaluation and therapeutic planning of developing patients. New longitudinal studies are needed to deepen the understanding of the mechanisms involved in this interaction and to strengthen the evidence related to preventive and therapeutic strategies applied to craniofacial growth.
References
-
R. E. Moyers, Handbook of Orthodontics. Chicago: Year Book Medical Publishers, 1988.
-
G. Castaldo and F. Cerritelli, “Craniofacial growth: evolving paradigms,” CRANIO, Vol. 33, No. 1, pp. 23–31, 2014, https://doi.org/10.1179/0886963414z.00000000042
-
N. Stimson and H. Jones, “Craniofacial development,” British Dental Journal, Vol. 235, pp. 583–589, 2023.
-
R. Capote, K. Preston, and H. Kapadia, “Craniofacial growth and development: a primer for the facial trauma surgeon,” Facial Plastic Surgery Clinics of North America, Vol. 31, No. 3, pp. 281–291, 2023, https://doi.org/10.1016/j.coms.2023.04.007
-
M. C. T. Pacheco, C. F. Casagrande, L. P. Teixeira, N. S. Finck, and M. T. M. Araújo, “Guidelines proposal for clinical recognition of mouth breathing children,” Dental Press Journal of Orthodontics, Vol. 20, No. 4, pp. 39–44, Aug. 2015, https://doi.org/10.1590/2176-9451.20.4.039-044.oar
-
C. Grippaudo et al., “Association between oral habits, mouth breathing and malocclusion,” Acta Otorhinolaryngologica Italica, Vol. 36, No. 5, pp. 386–394, 2016.
-
Z. Zhao, L. Zheng, X. Huang, C. Li, J. Liu, and Y. Hu, “Effects of mouth breathing on facial skeletal development in children: a systematic review and meta-analysis,” BMC Oral Health, Vol. 21, No. 1, p. 108, Mar. 2021, https://doi.org/10.1186/s12903-021-01458-7
-
Y.-S. Huang and C. Guilleminault, “Pediatric obstructive sleep apnea and the critical role of oral-facial growth: evidences,” Frontiers in Neurology, Vol. 3, Jan. 2013, https://doi.org/10.3389/fneur.2012.00184
-
J. Zhang, Y. Fu, L. Wang, and G. Wu, “Adenoid facies: a long-term vicious cycle of mouth breathing, adenoid hypertrophy, and atypical craniofacial development,” Frontiers in Public Health, Vol. 12, Dec. 2024, https://doi.org/10.3389/fpubh.2024.1494517
-
M. L. Moss, “The functional matrix hypothesis,” American Journal of Orthodontics, Vol. 48, No. 8, pp. 566–577, 1962.
-
M. L. Moss, “The functional matrix hypothesis revisited,” American Journal of Orthodontics and Dentofacial Orthopedics, Vol. 112, No. 1, pp. 8–11, 1997, https://doi.org/10.1016/s0889-5406(97)70265-8
-
D. H. Enlow and M. G. Hans, Essentials of Facial Growth. Philadelphia: W.B. Saunders, 1996.
-
R. C. Di Francesco, G. H. Passerotti, B. Paulucci, and S. Menta, “Mouth breathing in children: different repercussions according to the diagnosis,” Brazilian Journal of Otorhinolaryngology, 2004.
-
Y. Liu, J.-R. Zhou, S.-Q. Xie, X. Yang, and J.-L. Chen, “The effects of orofacial myofunctional therapy on children with OSAHS’s craniomaxillofacial growth: a systematic review,” Children, Vol. 10, No. 4, p. 670, Mar. 2023, https://doi.org/10.3390/children10040670
-
M. P. Villa and M. Evangelisti, “Orofacial myofunctional therapy for pediatric sleep disordered breathing,” in Snoring and obstructive sleep apnea in children, Elsevier, 2024, pp. 323–332, https://doi.org/10.1016/b978-0-323-99653-2.00021-3
-
E. S. Saba, H. Kim, P. Huynh, and N. Jiang, “Orofacial myofunctional therapy for obstructive sleep apnea: a systematic review and meta-analysis,” The Laryngoscope, Vol. 134, No. 1, pp. 480–495, 2023, https://doi.org/10.1002/lary.30974
-
W. A. Simões, Functional orthopedics of the jaws through neuro-occlusal rehabilitation. Porto Alegre: Artes Médicas, 2003.
About this article

The authors have not disclosed any funding.
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Gabriel Andrade Moreira de Assis: conceptualization, data curation, investigation, methodology, literature review, writing-original draft preparation, writing-review and editing. Isadora Stella Souza e Andrade: investigation, writing-original draft preparation, writing-review and editing. Lorena Gomes Marchant: investigation, writing-original draft preparation, writing-review and editing. Irene Acevedo: investigation, writing-original draft preparation, writing-review and editing. Márcia do Amaral Sampaio: methodology, writing-original draft preparation, writing-review and editing. Luciano Aparecido de Almeida-Junior: supervision, conceptualization, data curation, investigation, methodology, literature review, writing-original draft preparation, writing-review and editing.
The authors declare that they have no conflict of interest.
Present study consists of a narrative literature review based exclusively on previously published scientific data available in public databases (PubMed, SciELO, and Google Scholar).
As this study does not involve the direct collection of data from human or animal subjects, does not include clinical interventions, does not use biological samples, and does not access personal or confidential information of any individuals, it is exempt from submission to and approval by a Research Ethics Committee (REC/IRB), in accordance with the applicable national and international ethical guidelines governing scientific research.
All sources consulted were properly cited, and no individual or unpublished data were used without appropriate authorization.
