Abstract
The present study aims at presenting the impact of manual diaphragm relaxation therapy on the voice emission tested in an anechoic chamber and changes in the body posture during singing using the Zebris posturographic and pedobarographic platform. A pilot study on three cases has been conducted (patient 1 – male aged 21, student of the 2nd year of Academy of Music in Krakow, patient 2 – male aged 34, with more than 25 years of choral singing and advanced musical experience, patient 3 – female 24, with around 10 years of choral singing experience and primary musical school graduation). An original survey questionnaire was used, enabling determination the problematics associated with the profession of singer. A posturographic platform (Zebris) was used that revealed deviations during the scenic movement (by performing an appropriately developed repertoire). Subsequently, a voice emission examination was carried out in an anechoic chamber of the Department of Mechanics and Vibroacoustics, AGH University of Science and Technology. Directly after the examination, the examined individual was subject to a manual therapy lasting several minutes. The applied fascial techniques for diaphragm consisted in the implementation of a prolonged stretching of the myofascial complex with the use of low load. After the therapy, testing with the use of the aforementioned methods was repeated. The present study refers to the impact of the diaphragm function on voice emission parameters. In the pilot study for patient 1 and 2, 15 voice emission parameters improved. The analysis of the above results showed the variability before and after the diaphragm relaxation therapy in parameters such as Fo, Jitt and Shim. In the examined case of patient 1 and 2, the value of the parameter Jitt decreased by almost half, while Shim decreased by about 40 % after the therapy. However, such changes were not observed for patient 3. It may be influenced by many factors, such as stress or worse disposition on the day of the examination. The presented preliminary study expands the knowledge on the function of the diaphragm and the awareness of the function of ventilatory muscles during singing, which may result in enhanced efficiency of working with voice. In the future it is planned the study on bigger group students of Academy of Music in Krakow with the control group.
1. Introduction
Vocal prevention and hygiene should be the priority for teachers, choir conductors, singers etc. This is particularly important field that should be trained already at the lowest levels of education of work with voice. Studies on the impact of diaphragm on the body posture are also becoming increasingly common [1]. The biomechanical understanding of maintaining balance is considered as the capability of an individual to minimize the movement from the center of relative to the support plane. It has been proven that the diaphragm is activated in the phase of preparation to tasks that result in imbalance. It fulfills two functions at the same time: ventilation and stabilization. In the situation of increased ventilatory load diaphragm reduces the stabilization function. Vostatek et. al. demonstrated a significant relationship between the loss of stability of the lower part of the vertebral column relative to the increased demand for ventilation [2].
Voice emission is a process of producing and releasing voice externally. The process occurs due to coordinated actions: breathing, phonation, articulation and thus formed resonance [3]. The specificity of tissue connectivity due to fascial connections, by means of relaxation of the diaphragm, enables reducing the tension in the laryngeal area, which may contribute to correct impostation [4]. Aligning the pelvis in an intermediate position and correct loading of the knee and foot joints enable correct action of the diaphragm. Movement of the center of gravity posteriorly may result in increased lumbar lordosis and expansion of the abdominal muscles, whereas leaning backwards significantly disturb the movement of the chest [5]. The correct tension in the orofacial area is directly affected by the dynamic action and properly taut diaphragm. From the anatomical standpoint, it is a significant organ separating the abdominal cavity from the thoracic cavity [6]. It plays a significant role in maintaining the posture, understood as the torso stability and control during repeated motor function. The mentioned processes are highly dependent on the diaphragm function during ventilation, thus it can be concluded that it fulfills postural and ventilation function at the same time [7].
Singers are frequently unaware of the presence of acquired, unfavorable movements and improper tension of the muscles and tissues surrounding the larynx and diaphragm, which are associated with functional disorders of voice [8]. Individuals diagnosed with voice disorders show clavicular ventilation, which is inefficient from clinical standpoint and may be changed into being more efficient after physiotherapeutic intervention [9].
Professional classical singers are often in favor of active control of the abdominal cavity and of the thorax during performance. It is believed that this disables the diaphragm shortening, raises the thorax and thus contributes to a greater efficiency of subglottic pressure formation during phonation. However, these patterns have been quantitatively analyzed in only few studies, and the interpersonal variability has impeded identification of the stereotypical patterns of respiratory kinematics. It should be noted that the previous research demonstrated that in contrast to amateur singers, classical singers are characterized by a greater percentage contribution of the abdominal cavity in the lung volume during singing and the ability to desynchronize the movements of the thoracoabdominal movement. The movement of the abdominal press observed in classical singers affects the increase of pressure in the abdominal cavity. This phenomenon results in increased length and capability of thoracic expiratory muscles to produce pressure, which may enhance voice quality [10].
The described physiological process of subglottic pressure formation is highly significant for singers, but at the same time the disturbed balance of thoracic and abdominal press movement may lead to esophageal reflux. Gastroesophageal reflux is a condition caused by rapid change of the subglottic pressure in the abdominal cavity during diaphragm action, which results in increased intraabdominal pressure. The mentioned processes disable normal function of the diaphragm sphincter, as a result of which the mechanisms repeated over many years increase the likelihood of reflux incidence in singers [11].
It should be noted that the so-called Performance-Related Musculoskeletal Disorders (PRMD) can be observed among singers. Research shows that 79 % of singers experience PRMD before commencing music education at the university level. The incidence rate of PRMD is strongly correlated with the daily, long-hours of repeating the same movements, disturbed postural patterns, lack of proper work hygiene or the absence of regeneration strategies, as well as sedentary lifestyle [12].
The role of the fascia in human body is significant due to its common distribution and direct impact on healthy structures. The connective tissue forming fascia is a type of system, which by penetrating the muscles, nerves, blood vessels etc. forms a three-dimensional metabolic matrix. The lack of possibility displacement of fascia layers may have a significant impact on the quality of ergonomic physical activity. The structure of fascia is characterized by a considerable number of proprioceptors, which are located mainly in the areas between the fascia and contractile elements, such as muscles. What is more, fibroblasts forming the basis for the fascia, thanks to their capacity to change the vector, recreate the current mechanical vector, thus the transfer of the produced tension is more ergonomic and smoother. It has been proven that pathologic disturbance associated with the fascia system maintaining for a prolonged period of time may result in chronic muscle fatigue and pain [13].
2. Research material and methodology
A pilot study on three cases has been conducted (patient 1 – male aged 21, student of the 2nd year of Academy of Music in Krakow, patient 2 – male aged 34, with more than 25 years of choral singing and advanced musical experience, patient 3 – female 24, with around 10 years of choral singing experience and primary musical school graduation).
An original survey questionnaire was used, enabling determination the problematics associated with the profession of singer (i.a. pain of musculoskeletal origin, gastroesophageal reflux, resistance to stressful situations). A posturographic platform (Zebris) was used that revealed deviations during the scenic movement (by performing an appropriately developed repertoire). Subsequently, a voice emission examination was carried out in an anechoic chamber of the Department of Mechanics and Vibroacoustics, AGH University of Science and Technology. Directly after the examination, the examined individual was subject to a manual therapy lasting several minutes. The applied fascial techniques consisted in the implementation of a prolonged stretching of the myofascial complex of the diaphragm with the use of low load. In this manner, the domes and crura of the diaphragm were studied.
The person conducting the therapy sensed the most restricted direction of fascia displacement and applied pressure mobilization of soft tissues, directly on the skin and deeper in the fascia, until resistance was felt. Subsequently, the movement was stopped for several minutes, without displacement, until the fascia was relaxed (soft final resistance). The technique was coordinated with diaphragmatic breathing (Table 1). One series of each technique, 8 repetitions, time depends on individual breathing tempo. Break between each technique – 2 minutes. In physiotherapy techniques, therapist places palms under the osteochondral connections, thus stimulating ventilatory function [14].
2.1. Description of the techniques used
After the therapy, testing with the use of the aforementioned methods was repeated. Information sheet was given to patients and a verbal explanation of the nature of the study by the investigator. The patients agreed to participate in the study, an informed consent was signed. The study was conducted in accordance with the amended Declaration of Helsinki. Zebris FDM-S platform was used to assess stabilometric parameters of balance. The device was force-measuring platform with built-in capacitive force sensors enabling the measurement and analyses of force distribution under the feet (dimensions: 69×40×2.1 cm, Sensor surface: 54×33 cm, number of sensors: 2,560, sampling rate: 120 Hz). In assessing static stability, patients stood barefoot in a natural and relaxed position, with arms by the sides. During the assessment of stability, subject was asked to stay for 1 minute and test was repeated 3 times with a 5 sek. break. Volunteer completed the static balance task under two conditions: 1. test before myofascial techics, and 2. after treatment with 30 minutes break between each measurement.
Table 1The techniques for relaxation of diaphragm
No. | Starting position | Technique | Aim |
1. | Supine hook lying position | – Physiotherapist was turned towards subject’s head – Physiotherapist’s hands located laterally on subject’s chest with thumbs under costal arch – Study participant breathes calmly with diaphragm pattern – Next, while subject exhales, physiotherapist breaks soft tissue barrier with thumbs through deep myofascial relaxation – Physiotherapist with subject’s every exhale, move thumbs inferiorly (40-45 seconds, 8 repetitions) – At the end, physiotherapist slowly releases the grip | Relaxation of central tendon of diaphragm (diaphragmatic leaflets) |
2. | Supine hook lying position | – Physiotherapist is turned towards subject – Physiotherapist’s flat hands located laterally on subject’s chest (level of V-VIII rib) – Study participant breathes calmly from a diaphragm – Next, while subject exhales, physiotherapist press the chest resulting in deepening the exhale – Study participant performs inhale, while physiotherapist leaves hands in the same position, creating a resistance for subject’s inhale – After 2 seconds, physiotherapist releases the resistance, allowing patient to fully inhale | Relaxation of central tendon of diaphragm (diaphragmatic leaflets) |
3. | Sitting position on chair without back support, lower limbs 90 degrees flexed, hands on knees | – Physiotherapist sits behind study participant – Physioterapist’s hands located on posterior wall of subject’s chest with thumbs under costal arch in the area of erector spinae muscles – Study participant breathes calmly from a diaphragm – Next, while subject exhales, physiotherapist breaks soft tissue barrier with thumbs located under costal arch through deep myofascial relaxation – Physiotherapist with subject’s every exhale, move thumbs inferiorly (40-45 seconds, 8 repetitions) – At the end, physiotherapist slowly releases the grip | Relaxation of posterior branch of diaphragm |
The following stabilometric quantitative parameters were considered: path (total length of center of gravity displacement), ellipse (area in which the center of gravity oscillates), left and right side loading, back and fore side loading.
2.2. Singin procedure
The singing procedure is consisted of basic vocal exercises that was designed in order to observe the basic features of voice emission. In particular, the experiment was to analyze the relative quantity of tonal stability and musical dynamics within one long note. The procedure was performed before and after diaphragm muscle relaxation therapy to determine if there are any changes in the quality of the produced sound and what is their magnitude. The scheme of the singing exercises is shown in the Fig. 1.
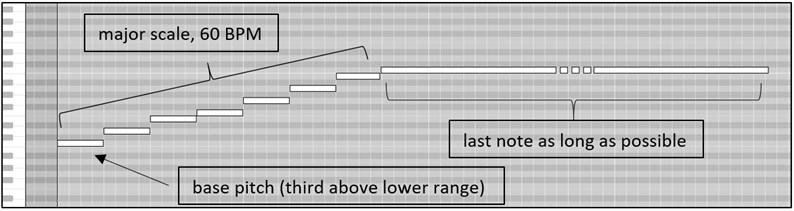
The consecutive stages of the procedure are illustrated by the logical blocks. The chosen vocal exercises are very basic and simple so each singer could focus on the sound emission only, and not pay any attention on the musical aspects or the exercises content. The first stage of recording voice was a rough identifying of the vocal range so the following exercises were performed in a convenient register for each singer individually. The second exercise (Fig. 2) was to sing major scale in a tempo of about 60 BPM (Beats Per Minute), with solmization in mf dynamics (it. mezzoforte: medium loud), starting a third (three semitones) above the previously determined lower range of the vocal range. The subjects were instructed to do this exercise in one breath and sing the last, highest note as long as possible.
Fig. 1Scheme of singing procedure to establish tonal and dynamic quality of the voice before and after the therapy

The next exercises were to sing simple single tones, in a most comfortable vowel for a particular singer, in one breath. Each pitch was singing in three different dynamics: p, mf, f (it. piano, forte: softly, loud). The person conducting the experiment before every round gave the base notes pitches in relation to the previously measured vocal range, i.e. in its low range (third above the bottom of the range), in the middle of the range and in the high range (third below the designated top of the scale). In every case, the subject task was to keep the sound stable and steady as long as possible, in the given pitch and dynamics.
Fig. 2Major scale singing in a 60 BPM, with solmization and mf dynamics
2.3. Voice emission recording and parametrization
The time-dependent acoustic speech signal was recorded in an anechoic chamber [16], at the Department of Mechanics and Vibroacoustic, AGH University of Science and Technology, Krakow, Poland. The diagram of the measurement setup is shown in Fig. 3. The applied professional registration system provided a transfer band from 20 Hz to 20 kHz at the dynamics amounted to not less than 80 dB.
The registered research material (described in 2.2) has been used for creation of a database, containing acoustic signal samples, recorded in the “wave” format. The impact of muscle relaxation therapy on voice emission has been based on parameters resulting from changes of the primary tone function – . The respective parameters have been divided into following groups with respect to [17]:
– base frequency (Fo, Fhi, Flo, T0, PFR, STD),
– fluctuation of the base frequency (Jitta, Jitt, PPQ, RAP, sPPQ, vF0),
– fluctuation of signal amplitude (ShdB, Shimm, APQ, sAPQ, vAm),
– variation of the signal’s time sections (NSH, NUV, NVB, DSH, DUV, DVB)
– noise present in the signal (VTI, SPI, NHR)
– tremble (Fatr, Fftr, ATRI, FTRI).
Fig. 3The block diagram of the measuring setup, where: 40 AF – G.R.A.S microphone, 1201 – NORSONIC preamplifier, 12AA – G.R.A.S amplifier, 1314 – M-AUDIO IN/OUT chart, PC – computer with Adobe Audition 3.0 software

3. Results
The acoustic signal parametrization was performed in the MDVP software package, offered by KAY ELEMETRICS [16].
Table 2Comparison of signal parameters before and after manual therapy for patient no. 1. Vowel with prolonged phonation – “a”
Parameter | Shortcut | Value | Unit | |
Before | After | |||
Average fundamental frequency | Fo | 187.43 | 186.38 | Hz |
Mean fundamental frequency | MFo | 187.35 | 186.34 | Hz |
Average pitch period | To | 5.33 | 5.36 | ms |
Highest fundamental frequency | Fhi | 204.25 | 194.99 | Hz |
Lowest fundamental frequency | Flo | 163.71 | 175.91 | Hz |
Standard deviation of Fo | STD | 3.94 | 2.68 | Hz |
Phonatory Fo-Range in semi-tones | PFR | 5 | 2 | |
Fo-tremor frequency | Fftr | 5.33 | 5.55 | Hz |
Amplitude tremor frequency | Fatr | 5.47 | 5.63 | Hz |
Length of analyzed sample | Tsam | 9.33 | 5.88 | s |
Absolute jitter | Jita | 44.19 | 24.36 | µs |
Jitter percent | Jitt | 0.83 | 0.45 | % |
Relative average perturbation | RAP | 0.51 | 0.24 | % |
Pitch perturbation quotient | PPQ | 0.36 | 0.22 | % |
Smoothed pitch perturbation quotient | sPPQ | 1.64 | 1.25 | % |
Fundamental frequency variation | vFo | 2.10 | 1.44 | % |
Shimmer in dB | ShdB | 0.23 | 0.14 | dB |
Shimmer percent | Shim | 2.77 | 1.69 | % |
Amplitude perturbation quotient | APQ | 1.91 | 1.34 | % |
Smoothed ampl. Perturbation quotient | sAPQ | 4.84 | 4.82 | % |
Peak-to-Peak Amplitude Variation | vAm | 15.10 | 12.36 | % |
Noise to Harmonic Ratio | NHR | 0.14 | 0.13 | |
Voice turbulence index | VTI | 0.04 | 0.06 | |
Soft phonation index | SPI | 3.62 | 3.14 | |
Fo-tremor intensity index | FTRI | 1.26 | 0.98 | % |
Amplitude tremor intensity index | ATRI | 5.07 | 5.50 | % |
In the pilot study for patient 1 and 2, 15 voice emission parameters improved. The analysis of the above results showed the variability before and after the diaphragm relaxation therapy in parameters such as Fo, Jitt and Shim [18]. Fo is the frequency of the fundamental vocal fold vibrations, while the Jitt parameter measures the cycle-to-cycle variation of this frequency, and the Shim parameter – the variability of the amplitude of the fundamental frequency of the vocal fold vibration during phonation. The Jitt and Shim values closer to zero indicate more effective work of the vocal folds through greater laryngeal stabilization. In the examined case of patient 1 and 2, the value of the parameter Jitt decreased by almost half, while Shim decreased by about 40 % after the therapy. However, such changes were not observed for patient 3. It may be influenced by many factors, such as stress or worse disposition on the day of the examination.
Table 3Comparison of signal parameters before and after manual therapy for patient no. 2. Vowel with prolonged phonation – “a”
Parameter | Shortcut | Value | Unit | |
Before | After | |||
Average fundamental frequency | Fo | 179.13 | 177.99 | Hz |
Mean fundamental frequency | MFo | 179.09 | 177.96 | Hz |
Average pitch period | To | 5.58 | 5.619 | ms |
Highest fundamental frequency | Fhi | 190.34 | 189.62 | Hz |
Lowest fundamental frequency | Flo | 166.53 | 132.52 | Hz |
Standard deviation of Fo | STD | 2.66 | 2.56 | Hz |
Phonatory Fo-range in semi-tones | PFR | 3 | 7 | |
Fo-tremor frequency | Fftr | 4.87 | 4.93 | Hz |
Amplitude tremor frequency | Fatr | 4.87 | 5.12 | Hz |
Length of Analyzed Sample | Tsam | 11.18 | 13.31 | s |
Absolute jitter | Jita | 47.40 | 35.34 | µs |
Jitter percent | Jitt | 0.84 | 0.62 | % |
Relative average perturbation | RAP | 0.49 | 0.39 | % |
Pitch perturbation quotient | PPQ | 0.46 | 0.30 | % |
Smoothed pitch perturbation quotient | sPPQ | 1.05 | 0.73 | % |
Fundamental frequency variation | vFo | 1.48 | 1.44 | % |
Shimmer in dB | ShdB | 0.25 | 0.16 | dB |
Shimmer percent | Shim | 3.26 | 1.85 | % |
Amplitude perturbation quotient | APQ | 2.16 | 1.39 | % |
Smoothed ampl. Perturbation quotient | sAPQ | 5.23 | 4.36 | % |
Peak-to-peak amplitude variation | vAm | 22.51 | 23.82 | % |
Noise to harmonic ratio | NHR | 0.13 | 0.12 | |
Voice turbulence index | VTI | 0.03 | 0.02 | |
Soft phonation index | SPI | 15.73 | 11.41 | |
Fo-tremor intensity index | FTRI | 0.72 | 0.47 | % |
Amplitude tremor intensity index | ATRI | 5.37 | 3.96 | % |
For patient 1 and 2, the same four parameters improved compared to their values before the therapy. The parameters STD and vFo are responsible for the values of the standard deviation of the fundamental frequency in the analyzed voice sample. Their improvement means that the frequency values in the entire signal are closer to the average fundamental frequency of the analyzed signal. The signal is less fluctuating than before therapy, which affects sound quality. The other two parameters (DUV and NUV), the values of which improved in patient 1 and 2, describe the degree of silence, i.e. the relative assessment of non-harmonic areas in the sample and the number of silent sections in the signal, which shows the better ability of the subject to continue talking (singing) after manual therapy. It is planned that the study will cover approximately 30 students of Academy of Music in Krakow, aged 19-26. The control group will consist of people aged 19-26 practicing singing at an amateur level.
4. Conclusions
The essence of taking care of voice hygiene is the knowledge of risk factors for the development of voice pathology in people who use voice on a daily basis during their professional duties. Research shows that the development of voice disorders is affected by, among others: age, sex, but also individual personal factors such as the duration and frequency of using voice throughout the day, number of performances, habitual chin extension, leaning during singing [15]. The present study refers to the impact of the diaphragm function on voice emission parameters. In the future it is planned the study on bigger group students of Academy of Music in Krakow with the control group.
Table 4Comparison of signal parameters before and after manual therapy for patient no. 3. Vowel with prolonged phonation – “a”
Parameter | Shortcut | Value | Unit | |
Before | After | |||
Average fundamental frequency | Fo | 365.03 | 345.78 | Hz |
Mean fundamental frequency | MFo | 364.99 | 345.72 | Hz |
Average pitch period | To | 2.740 | 2.892 | ms |
Highest fundamental frequency | Fhi | 398.96 | 389.62 | Hz |
Lowest fundamental frequency | Flo | 335.51 | 329.18 | Hz |
Standard deviation of Fo | STD | 3.73 | 4.28 | Hz |
Phonatory Fo-range in semi-tones | PFR | 4 | 4 | |
Fo-tremor frequency | Fftr | 2.51 | 5.40 | Hz |
Amplitude tremor frequency | Fatr | 4.87 | 5.33 | Hz |
Length of Analyzed Sample | Tsam | 6.43 | 6.19 | s |
Absolute jitter | Jita | 8.52 | 40.40 | µs |
Jitter percent | Jitt | 0.31 | 1.39 | % |
Relative average perturbation | RAP | 0.18 | 0.92 | % |
Pitch perturbation quotient | PPQ | 0.16 | 0.58 | % |
Smoothed pitch perturbation quotient | sPPQ | 0.53 | 0.87 | % |
Fundamental frequency variation | vFo | 1.02 | 1.23 | % |
Shimmer in dB | ShdB | 0.10 | 0.63 | dB |
Shimmer percent | Shim | 1.10 | 7.35 | % |
Amplitude perturbation quotient | APQ | 0.82 | 4.06 | % |
Smoothed ampl. perturbation quotient | sAPQ | 4.27 | 8.13 | % |
Peak-to-peak amplitude variation | vAm | 14.00 | 15.12 | % |
Noise to harmonic ratio | NHR | 0.09 | 0.11 | |
Voice turbulence index | VTI | 0.03 | 0.02 | |
Soft phonation index | SPI | 13.35 | 14.90 | |
Fo-tremor intensity index | FTRI | 0.46 | 0.54 | % |
Amplitude tremor intensity index | ATRI | 6.19 | 8.05 | % |
References
-
Kocjan J., Gzik Zroska B., et al. Impact of diaphragm function parameters on balance maintenance. PLoS One, Vol. 13, Issue 12, 2018, p. e0208697.
-
Vostatek Novák P. D. Diaphragm postural function analysis using magnetic resonance imaging. PLoS One, Vol. 8 Issue 3, 2013, p. e56724.
-
Wojtaszek A. Prevention and Voice Hygiene in Music Education in Children and Young People. Psychological-Pedagogical Notebooks of Artistic Education Centre, 2015, (in Polish).
-
Marszałek S., Niebudek Bogusz E., Woźnicka E., Kowalska M. Ś. The application of physiotherapeutic and ostheopatic diagnostics in ocuppational voice disorders. Occupational Medicine, Vol. 61, Issue 2, 2010, p. 205-211, (in Polish).
-
Sadowska, Dragun, Gutowska, Szczepaniak R. The meaning of the right body posture during speech therapy. Speech-Therapy Forum, Vol. 24, 2016, p. 59-70, (in Polish).
-
Snell R. S. Clinical Anatomy by Regions. Philadelphia, Lippincott Williams and Wilkins, 2008.
-
Kocjan J., Adamek M., Gzik Zroska B., Rydel M. Network of breathing. Multifunctional role of the diaphragm: a review. Advances in Respiratory Medicine, Vol. 85, 2017, p. 224-232.
-
Sielska Badurek E., Domeracka Kołodziej A. Evaluation of breath support in classical singing. Otorhinolaryngology, Vol. 8, Issue 3, 2009, (in Polish).
-
Murray E. S. H., Michener C. M., Enflo L., Cler G. J., Stepp C. E. The impact of glottal configuration on speech breathing. Journal of Voice, Vol. 32, Issue 4, 2018, p. 420-427.
-
Salomoni S., Van Den Hoorn W., Hodges P. Breathing and singing: objective characterization of breathing patterns in classical singers. PLoS ONE, Vol. 11, Issue 5, 2016, p. e0155084.
-
Loor A., Nedelcut S., Dumitrascu D. L. High prevalence of gastroesophageal reflux in vocal opera students. A case-control type study. Medicine and Pharmacy Reports, Vol. 93, Issue 2, 2020, p. 145-149.
-
Śmieszchalska J. Prevention of ailments resulting from specificity of playing musical instruments – new challenge for teachers. Psychological-Pedagogical Notebooks of Artistic Education Centre, 2015, p. 55-68, (in Polish).
-
Bordoni B., Marelli F. The fascial system and exercise intolerance in patients with chronic heart failure: hypothesis of osteopathic treatment. Journal of Multidisciplinary Healthcare, Vol. 8, 2015, p. 489-494.
-
Bordoni B., Marelli F., et al. Manual evaluation of the diaphragm muscle. International Journal of Chronic Obstructive Pulmonary Disease, Vol. 11, 2016, p. 1949-1956.
-
Phyland D., Miles A. Occupational voice is a work in progress: active risk management, habilitation and rehabilitation. Current Opinion in Otolaryngology and Head and Neck Surgery, Vol. 27, Issue 6, 2019, p. 439-447.
-
Wierzbicki J., Małecki P., Wiciak J. Localization of the sound source with the use of the first-order ambisonic microphone. Acta Physica Polonica. A, Vol. 123, Issue 6, 2013, p. 1114-1117.
-
Kay Elemetrics: Multi-Dimensional Voice Program (MDVP) 5015 Software Instruction Manual. New Jork, 2005.
-
Kłaczyński M. Vibroacoustic methods in diagnosis of selected laryngeal diseases. Journal of Vibroengineering, Vol. 17, Issue 4, 2015, p. 2089-2098.
About this article

This research has been partly supported by AGH UST project No. 16.16.130.942.
Special thanks to the professor Zdzisław Madej, head of Voice Department at Academy of Music in Krakow.
