Abstract
Dental topography can be defined as the division of receptive fields that we have in the crown of the tooth. It is necessary that we understand this concept very well because it makes all the difference in clinical practice. We need to understand the receptive fields of the tooth, and we must use this knowledge when prescribing accessories for a functional appliance, understanding its function and where these accessories should touch to generate the expected effect. In this paper we will discuss the fundamentals of dental topography and show some accessories used on the therapeutic arsenal of Jaw Functional Orthopedics.
Highlights
- The touch sensibility of the teeth are extremely high.
- The brain is able to sense and discriminate the touch in different fields of the crown.
- The efferent answer coming from the brain will be different according to the field stimulated.
- Functional appliances accessories are not springs that push teeth.
- Functional appliances accessories touch the teeth to generate sensorial afferences.
- The choice of accessories and where they must touch ensure the results of the treatment.
1. Introduction
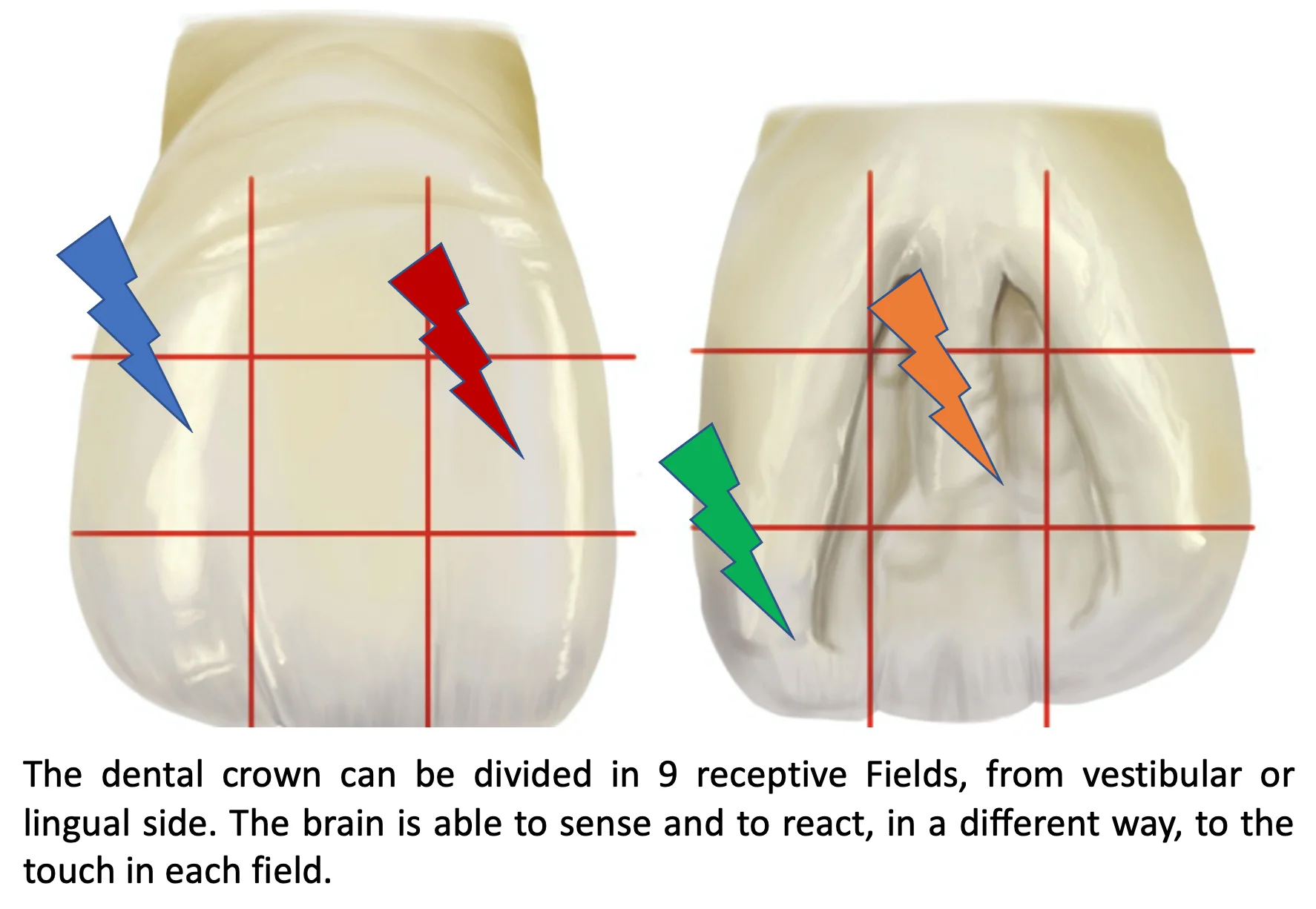
Tooth is a rigid structure connected to extremely sensitive soft structures. A slight mechanical disturbance in the enamel can be perceived in exquisite detail by the periodontal ligament [1, 2] and the pulp[3] And the discriminative capacity is so great that we can sectorize the dental crown [1, 2]. The division of thirds in the dental crown, vertically, follows the pattern of the columns of tooth formation that end up generating mamelons [4]. Differentiated receptive fields are generated both vestibular and lingual. Horizontally, we can divide the crown into cervical, middle, and incisal thirds (Fig. 1). In this way, we can didactically establish 9 receptive fields in the crown of the tooth. These receptive fields refer to the sensations perceived by the pulp and mainly by the periodontal ligament. The touch performed on the crown propagates through the laws of physics (which can be quantified with finite element studies), and can thus be perceived, as mentioned, by the nerve endings of the pulp and periodontium [5, 6].
Fig. 1The dental crown can be divided in 9 receptive fields. We must consider on a vertical division, the establishment of a mesial third, a medium third and a distal third. Considering a horizontal division, we will have a cervical third, a medium third and an incisal third
The periodontal ligament has a hydraulic system that is highly sensitive to any mechanical disturbance, having inside it the presence of specific axonal specializations that can perceive minimal stimuli and generate afferents to the CNS [7]. The tooth perceptive ability starts with first temporary incisor eruption and reaches its maturity after the eruption of the second molar. Depending on the location of the mechanical disturbance and the age of the individual, the remodeling response will be different because the density of receptors varies not only from tooth to tooth, as in the same tooth varies from region to region, When these different afferents reach the central nervous system, they will generate different motor outputs for the muscles (which are being controlled in postural terms by the periodontal ligament), and we must remember that muscles control bone remodeling [8-10]. Other important aspect is that brain representation, both at the level of Gasserian ganglion or at the level of the mesencephalic nucleus is greater in the incisors and do to that we are always trying to achieve DA (Determined Area), to amplify the afferences to the CNS [11, 12]. Having all these considerations in mind, it is extremely important that the appliance confection and accessories placement follows strict rules, and some details must be considered:
1) Accessories are bent pieces of wire, with pre-determined designs, added to functional appliances as a resource to obtain specific therapeutic answers. They can never negatively influence the therapeutic posture changing (TPC) of this appliance.
2) Modifications are some alterations made on a given appliance to individualize the therapeutic purpose. The operational base, the structure and the fundamental components of the original appliance must be always kept without any modification.
2. Clinical relevance
Jaw Functional Orthopedics is not removable orthodontics. The functional appliances way of working is based on the generation of different afferences (neural excitation), to change the motor efferences and, in consequence, lead to change on bone remodeling. Due to that, the correct planning and placement of accessories that will lead to desirable afferences, are critical for an effective clinical approach.
3. Relevant accessories
Some important points on accessories confection are shown here, and it is necessary to reinforce that, for any given accessory, the placement of the bends must respect the therapeutic objective. It means that, the specialist must draw for the technician construct. To understand this, let’s see an important example:
3.1. Ondulating propulsion arch
Modification of the Bimler vestibular arch with the purpose of touching specific areas of the crown, to generate remodeling and consequent alignment Fig. 2.
Fig. 2a) Scheme of confection of an Ondulating Propulsing Arch. Observe that the measurements must be respected because they take in account the clinical observations of Simões. b) The nine topographic places must be observed
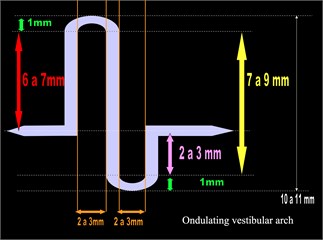
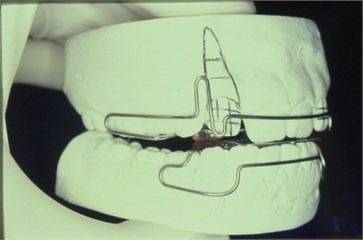
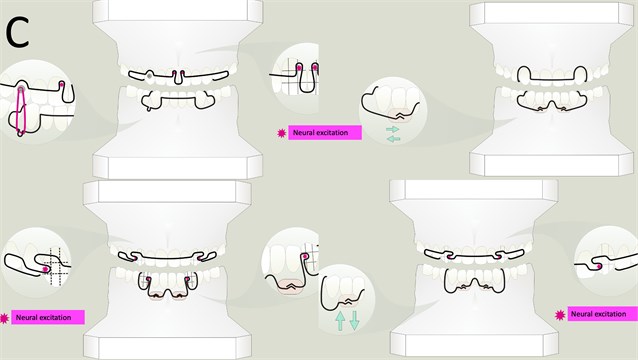
Fig. 3DHC arch designs. Observe that in all panels, the star shows the dental neural excitation respecting the crown topography
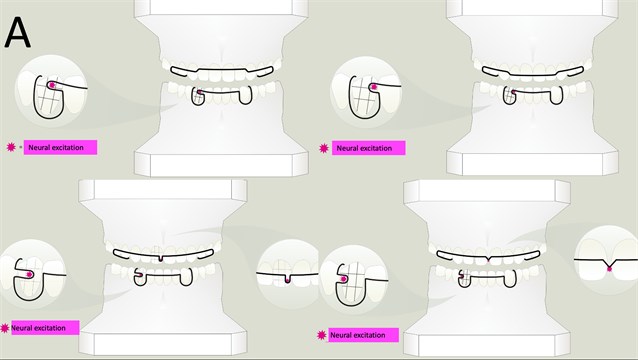
a) Different possibilities for touching one of the nine sites of the crown
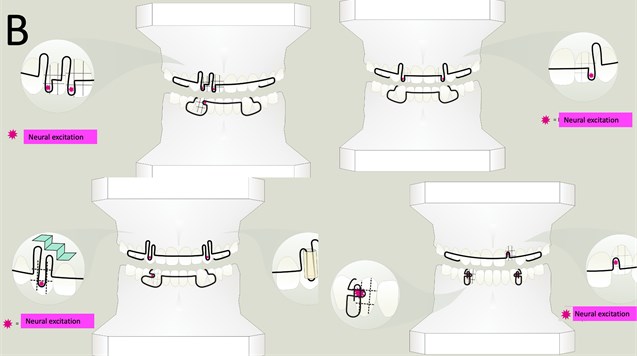
b) Four different possibilities of arch folding enhancing flexibility and generating multiple neural excitation points
c) Vestibular arch folding can be used as anchorage for traction (superior left), as support for shields (sup right). Observe that the design of the vestibular arch influences the minimum movement made by the shield. On inferior figures, different possibilities of folding, to generate neural excitation on superior and inferior vestibular arch
d) Different possibilities of Eschler arch modification. On the schemes where stars are not highlighted, the accessory was designed to reinforce the anchorage of posture changing
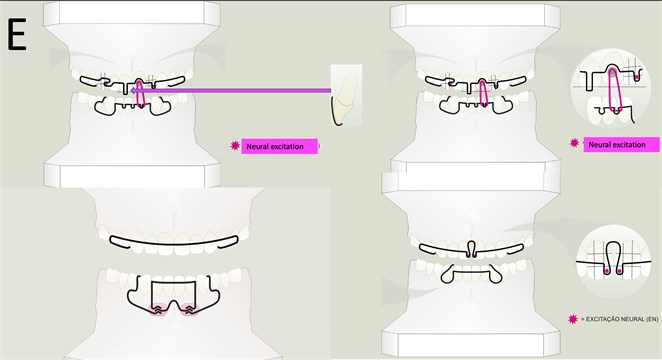
e) Different designs for different purposes. On upper images, intrusion (left) and traction (right) design. On lower images, mandible, and incisors anchorage (left) and neural excitation for two central incisors mesial lingualizing (right)
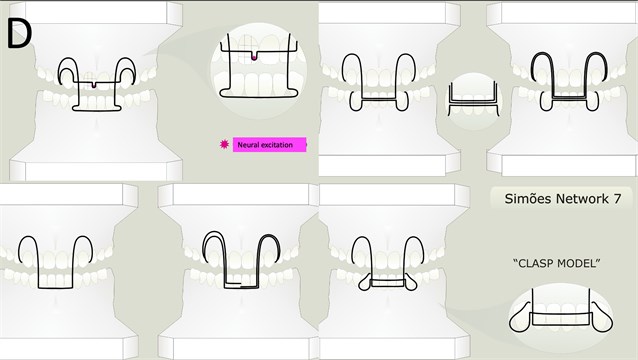
3.2. Different types of vestibular arch designed by Simões [11] and the first author
Sometimes, to achieve the therapeutic goal, it is necessary to create modifications on vestibular arch generating specific designs. Always respecting the crown topography, each folding aims to amplify the dental neural excitation or to anchor the posture changing. According to Simões principles, the first author of this article, developed important designs for vestibular arch, that will be shown on 5 panels of the Fig. 3.
4. Discussion
Despite not having nerve endings in its structure, enamel perceives mechanical stimuli in two ways:
1) The mechanical signal propagates to the amelodentinal limit and there activates the sensory fibers present in the dentinal canaliculi [3].
2) The propagated mechanical signal excites the highly discriminative nerve endings of the periodontal ligament [2, 13, 14].
Therefore, any touch exerted on the crown, even being minimal, will be perceived, because it generates a disturbance in the nerve fibers of the pulp and/or periodontal ligament. An important issue is the fact that fibers and receptors have different densities in each tooth. Anterior teeth have a larger population of receptors that decrease until the molars [15, 16]. We must also remember that there is a difference in perception, depending on whether these fibers are more cervical, median, or apical [17, 18], and the motor response generated will consequently be different. There is also a difference in the density of nerve fibers and receptors if we consider the primary and permanent dentition [19]. The perceptive ability matures and reaches its fullness after the eruption of the second molar. This means that, depending on the location of the mechanical disturbance and the age of the individual, the remodeling response will be different.
5. Conclusions
Accessories used in functional appliances are not springs to push or pull teeth. They are mechanisms specifically designed to generate neural excitation directly touching specific points of teeth crown or helping to anchor the posture changing generated by the appliances.
References
-
M. Trulsson, R. S. Johansson, and K. A. Olsson, “Directional sensitivity of human periodontal mechanoreceptive afferents to forces applied to the teeth,” The Journal of Physiology, Vol. 447, No. 1, pp. 373–389, Feb. 1992, https://doi.org/10.1113/jphysiol.1992.sp019007
-
T. Toda and M. Taoka, “The complexity of receptive fields of periodontal mechanoreceptive neurons in the postcentral area 2 of conscious macaque monkey brains,” Archives of Oral Biology, Vol. 46, No. 11, pp. 1079–1084, Nov. 2001, https://doi.org/10.1016/s0003-9969(01)00076-0
-
M. R. Byers, “Chewing causes rapid changes in immunoreactive nerve patterns in rat molar teeth: Implications for dental proprioception and pain,” Archives of Oral Biology, Vol. 107, p. 104511, Nov. 2019, https://doi.org/10.1016/j.archoralbio.2019.104511
-
E. S. Negra and O. L. Oliveira, “Polymorphism of the crown of the human maxillary permanent lateral incisor,” (in Portuguese), Arquivos do Centro de Estudos do curso de odontologia, Vol. 19, No. 2, pp. 215–26, 1982.
-
C. Yu and P. Abbott, “An overview of the dental pulp: its functions and responses to injury,” Australian Dental Journal, Vol. 52, pp. S4–S6, Mar. 2007, https://doi.org/10.1111/j.1834-7819.2007.tb00525.x
-
S. Jakupovic, E. Cerjakovic, A. Topcic, M. Ajanovic, A. Konjhodzicprcic, and A. Vukovic, “Analysis of the Abfraction Lesions Formation Mechanism by the Finite Element Method,” Acta Informatica Medica, Vol. 22, No. 4, p. 241, 2014, https://doi.org/10.5455/aim.2014.22.241-245
-
Y. Morimoto et al., “Effect of transient occlusal loading on the threshold of tooth tactile sensation perception for tapping like the impulsive stimulation,” Odontology, Vol. 101, No. 2, pp. 199–203, Jul. 2013, https://doi.org/10.1007/s10266-012-0072-3
-
J. Zhong et al., “Microstructural heterogeneity of the collagenous network in the loaded and unloaded periodontal ligament and its biomechanical implications,” Journal of Structural Biology, Vol. 213, No. 3, p. 107772, Sep. 2021, https://doi.org/10.1016/j.jsb.2021.107772
-
Hellsing G., “Human jaw muscle motor behaviour. II. Reflex and receptor mechanisms,” Swedish dental journal, Vol. 12, No. 1-2, pp. 47–56, 1988.
-
F. Pei et al., “Corrigendum to “The functions of mechanosensitive ion channels in tooth and bone tissues,” Cellular Signalling, Vol. 92, p. 110276, Apr. 2022, https://doi.org/10.1016/j.cellsig.2022.110276
-
Simões W. A., Ortopedia Funzionale dei Mascellari. Attraverso la Riabilitazione Neuro – Oclusale. 2010.
-
T. Maeda, “Sensory innervation of the periodontal ligament in the incisor and molar of the monkey, Macaca fuscata. An immunohistochemical study for neurofilament protein and glia-specific S-100 protein,” Archivum Histologicum Japonicum, Vol. 50, No. 4, pp. 437–454, 1987, https://doi.org/10.1679/aohc.50.437
-
T. Maeda, K. Kannari, O. Sato, and T. Iwanaga, “Nerve terminals in human periodontal ligament as demonstrated by immunohistochemistry for neurofilament protein (NFP) and S-100 Protein,” Archives of Histology and Cytology, Vol. 53, No. 3, pp. 259–265, 1990, https://doi.org/10.1679/aohc.53.259
-
T. Maeda, K. Ochi, K. Nakakura-Ohshima, S. H. Youn, and S. Wakisaka, “The Ruffini ending as the primary mechanoreceptor in the periodontal ligament: its morphology, cytochemical features, regeneration, and development,” Critical Reviews in Oral Biology and Medicine, Vol. 10, No. 3, pp. 307–327, Jun. 1999, https://doi.org/10.1177/10454411990100030401
-
E. Goellner and C.E. Rocha, “Anatomy of trigeminal neuromodulation targets: from periphery to the brain,” Progress in Neurological Surgery, Vol. 35, pp. 18–34, 2020, https://doi.org/10.1159/000511257
-
M. Trulsson, “Sensory-motor function of human periodontal mechanoreceptors,” Journal of Oral Rehabilitation, Vol. 33, No. 4, pp. 262–273, Apr. 2006, https://doi.org/10.1111/j.1365-2842.2006.01629.x
-
S. E. Johnsen and M. Trulsson, “Encoding of amplitude and rate of tooth loads by human periodontal afferents from premolar and molar teeth,” Journal of Neurophysiology, Vol. 93, No. 4, pp. 1889–1897, Apr. 2005, https://doi.org/10.1152/jn.00664.2004
-
R. Jacobs and D. Steenberghe, “Role of periodontal ligament receptors in the tactile function of teeth: a review,” Journal of Periodontal Research, Vol. 29, No. 3, pp. 153–167, May 1994, https://doi.org/10.1111/j.1600-0765.1994.tb01208.x
-
K. Miki, S. Honma, S. Ebara, K. Kumamoto, S. Murakami, and S. Wakisaka, “Changes in the distribution of periodontal nerve fibers during dentition transition in the cat,” PLOS ONE, Vol. 10, No. 6, p. e0129826, Jun. 2015, https://doi.org/10.1371/journal.pone.0129826
About this article

The authors would like to thank the technician Marcos Grivicic Pohl for the confection of the draws.
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
The authors declare that they have no conflict of interest.
