Abstract
Use of functional orthopedic appliances (FOA) in the treatment of malocclusion and Temporomandibular Disorders (TMD) has been proved to be effective but there is still questions to be answered like the muscular action of the referred appliances. The aim of this study is checking through a proven protocol of surface electromyography (sEMG) to study muscular action of FOA to check to check if it is correctly manufactured. The appliance studied is a Simões Network 10 – SN10 to treat Class II malocclusion of retrognathia. The sEMG was collected 1 patients with class II malocclusion with retrognathia who belong to a 164 volunteers with malocclusion, in two times T1 before installation of the FOA in mouth, T2 15 minutes after the FOA installation in the mouth. sEMG data of bilateral masseter, bilateral temporal and bilateral suprahyoid muscles using conditioner signals module from Lynx Electronics Ltda with 8 channels, model EMG1000; software AqDAnalysis 4,18 from Lynx Electronics Ltda.; Software Lynx BioInspector 1,8r; passive surface electrodes (Ag/AgCl) from Noraxon Dual Electrodes (USA); dischargeable reference electrodes Kendall Meditrace (Ag/AgCl) – Canada were used for the sEMG measurements. Frequency calibration was 2000 Hz, with 2048 sample by channel and time 1,024 seconds, and filters regulation was 20 Hz and 1000 Hz. With the FOA in the mouth all measurements improved with a more simetrical sEMG in T2 in rest and isometric contraction measurements. The protocol used to check the manufacturing of functional orthopedic appliances using surface EMG proved to be a valid tool in this case report study. Further investigations are needed to confirm this protocol and check if the same happens with other types of functional orthopedics appliances.
Highlights
- A New tool to check functional orthopedics appliances manufacture - sEMG
- Balancing stomatognathic muscle with jaw functional orthopedics
- Improvement of stomatognathic muscle function with functional orthopedic appliances - a sEMG measurement
- Use of sEMG in Jaw Functional Orthopedics
- Use of sEMG in dentistry
1. Introduction
Jaw Functional Orthopedics (JFO) is a growing field with very interesting clinical results in the treatment of malocclusion, dentofacial development problems [1-7] and Temporomandibular Disorders (TMD) [8,9], but still needs stronger scientific basis [10-12].
Information about the use of Bionator, Twin Block, Fränkel Function Regulators for class II treatment is available in the literature. O’Brien et al. [13] reported improvement in the antero posterior relationship of the mandible with use of Twin Block in Class II treatment and very positive psychosocial improvement of the teen agers due to facial esthetic improvement. Santamaria-Villegas et al. [14] in a systematic review reported that mandibular advancement with Twin Block, Bionator, Harvold Activator, Fränkel Functional Regulator and Sander Bite Jumping. Cozza et al. [15] reported the success of mandibular advancement in the treatment of classe II malocclusion, also in a systematic review that includes several types of functional appliances, some fixed as the Herbst, for instance, other removable like twin block, Fänkel regulator and so on.
None of the studies report improvement with Bimler, Planas, Simões and Santiago appliances. Despite the fact that these appliances very much used in Brazil have no RCT showing their efficiency, clinical results lead to try to understand what these appliances do with the stomatognathic muscles [16]. The in middle of the XX century, Moyers [17] reported the use of electromyography (EMG) to study the behavior of the stomatognathic muscles in class II malocclusion and their behavior in the mandibular movement [18].
Based on the results obtained by Sakai [16], the objective of this study is proposing a method using surface electromyography to check if manufactured Simões Network 10 – SN10 [19] is properly done.
2. Methods
One of the patients treated in the specialization course of Jaw Functional Orthopedics JFO, have prescription of the SN10. The treatment protocol includes diagnosis: Anamnesis, physical and Functional exams, lateral tele radiography with Bimler and Petrovic cephalometry, tele radiography in normal head position (NHP) with Rocabado Cephalometry), Planas Gnatostathic diagnostic protocol (casts and gnatostathic records), mouth and body photos and films. After completing the diagnosis, the 11 years old boy with Angle Class II, superior incisor protrusion received his functional orthopedic appliance (FOA). The therapeutic mandibular posture change (TMPC) was made advancing the mandible until the incisal third of the buccal surface of the inferior incisors touch the incisal third of the palatine surface of the superior incisors, this touch is called touch in determined area (DA) [19]. The FOA SN10 was chosen because the patent had a retrognathia and the vertical aspect is normal so the mandibular advancement does not need a significant vertical dimension increase. This can be the indication to prescribe the Simões Network 1 (SN1) [19] too. The election of the SN10 as due to three basic aspects: the range of the protrusive movement of the patient is short so it is interesting to use Fränkel anterior inferior pads of its adaptations [19] that is present in the SN10 FOA; the need for mandibular transversal stimulation was small, for such there was no need of an inferior expansion screw and the SN10 occupies less space on the mouth being more comfortable to the tongue improving use conditions of the FOA by the patient.
The sEMG was used because it is the better way to check the muscular activity behavior of the patient with the FOA and Sakai [16] protocol was used because it is able to register the studied muscles activity changes due to FOA use. It was collected in two times T1 before installation of the FOA in mouth, T2 15 minutes after the FOA installation in the mouth. sEMG data of bilateral masseter, bilateral temporal and bilateral suprahyoid muscles were done in three conditions: rest position of the mandible, isometric contraction with FOA and isometric contraction without FOA. The Ambiental conditions were controlled, especially electromagnetic area isolation, following ISEK protocol. A conditioner signals module from Lynx Electronics Ltda with 8 channels, model EMG1000; software AqDAnalysis 4,18 from Lynx Electronics Ltda.; Software Lynx BioInspector 1,8r; passive surface electrodes (Ag/AgCl) from Noraxon Dual Electrodes (USA); dischargeable reference electrodes Kendall Meditrace (Ag/AgCl) - Canada were used for the sEMG measurements. Frequency calibration was 2000 Hz, with 2048 sample by channel and time 1,024 seconds, and filters regulation was 20 Hz and 1000 Hz. No normalization analysis, were used and all sEMG signals were registered in T1 and T2 for 5 seconds. All tutors signed a free and informed consent form. The investigation was realized under the consent of Ethic Committee of Universidade Federal de Campinas (UNICAMP), Piracicaba, Brazil under protocol 159/2004. SN10 appliance were made following instructions contained on Simoes [19].
3. Results
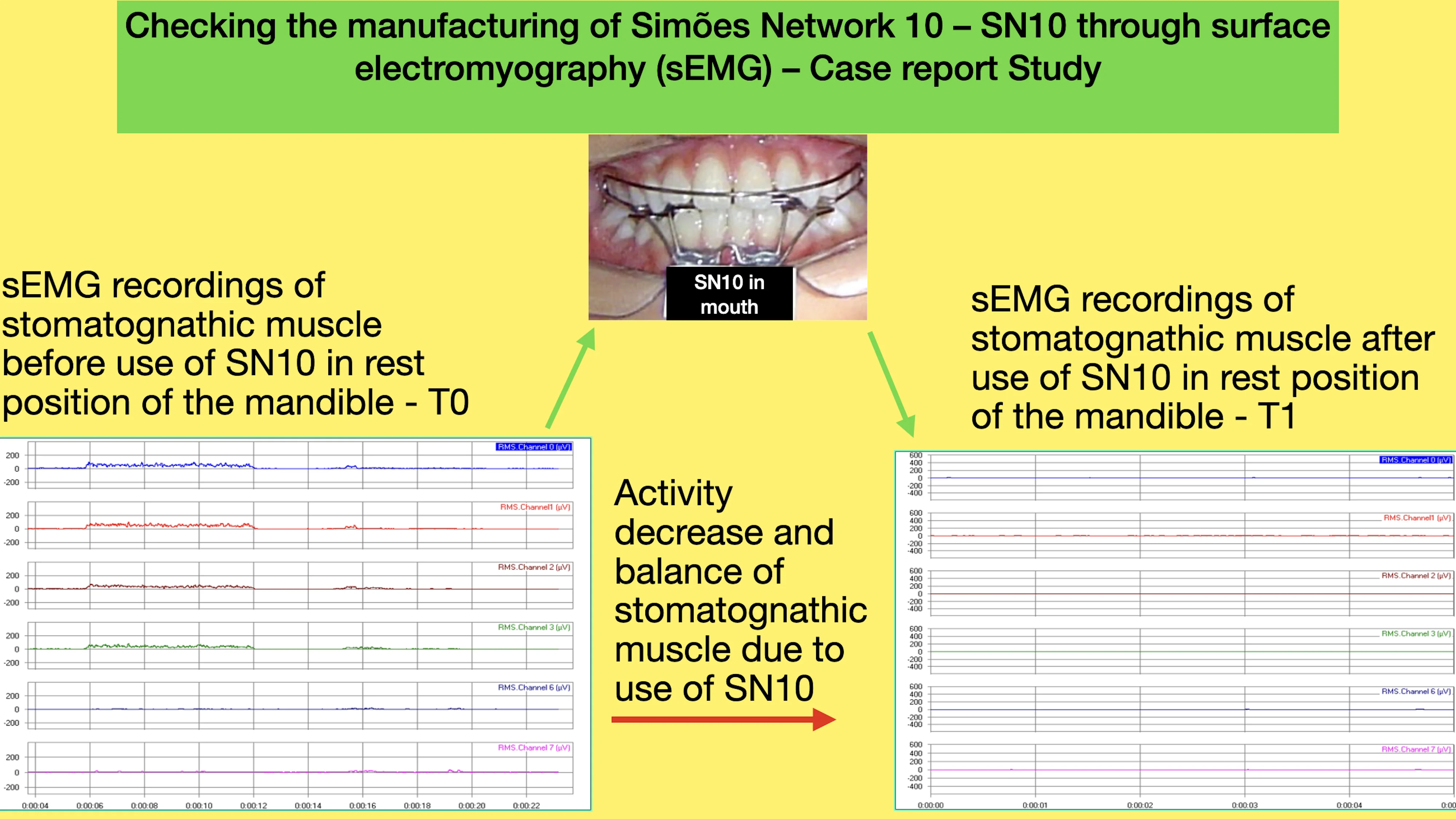
In the sEMg measurements showed in Figs. 1-4 the register of the electric activity of the right and masseter, right and left temporal, and right and left suprahyoid muscles. It can be observed the raise in electric activity of the muscles during isometric contraction with the FOA (T2) and the diminish of the muscle electric activity in the mandibular rest position with the FOA (T2).
Fig. 1Isometric contraction of the individual in T1. In light blue represents the electric activity of the right masseter, in red of the left masseter, in wine color electric of right temporal, in green of the left temporal, in dark blue of the right suprahyoid and in pink of the left suprahyoid
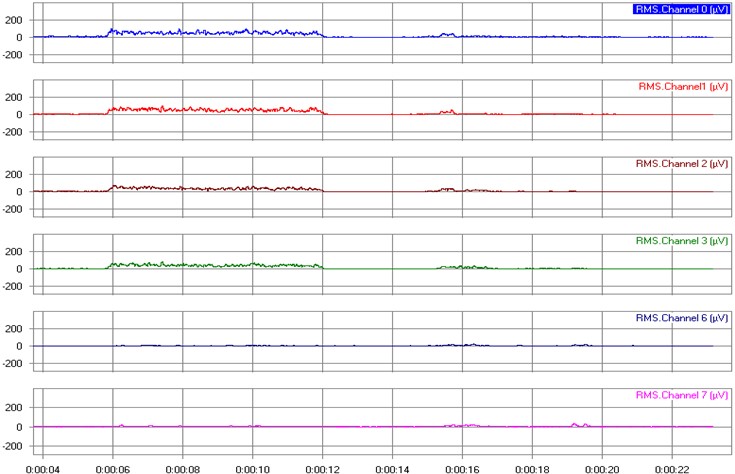
Fig. 2sEMG of the individual in rest position in T1. In light blue represents the electric activity of the right masseter, in red of the left masseter, in wine color electric of right temporal, in green of the left temporal, in dark blue of the right suprahyoid and in pink of the left suprahyoid
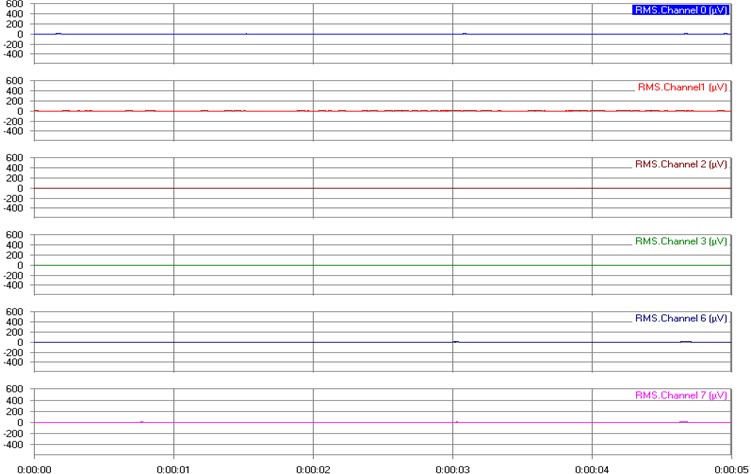
Fig. 3sEMG register of isometric contraction of the individual in T2
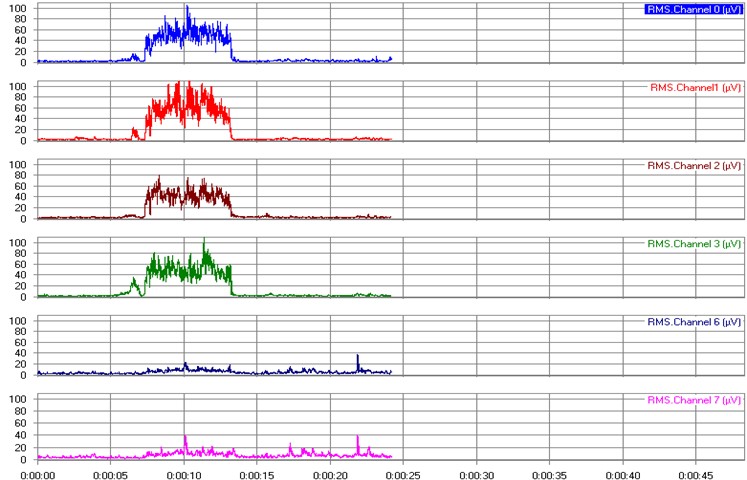
Fig. 4sEMG of the individual in mandibular rest position in T2. In light blue represents the electric activity of the right masseter, in red of the left masseter, in wine color electric of right temporal, in green of the left temporal, in dark blue of the right suprahyoid and in pink of the left suprahyoid
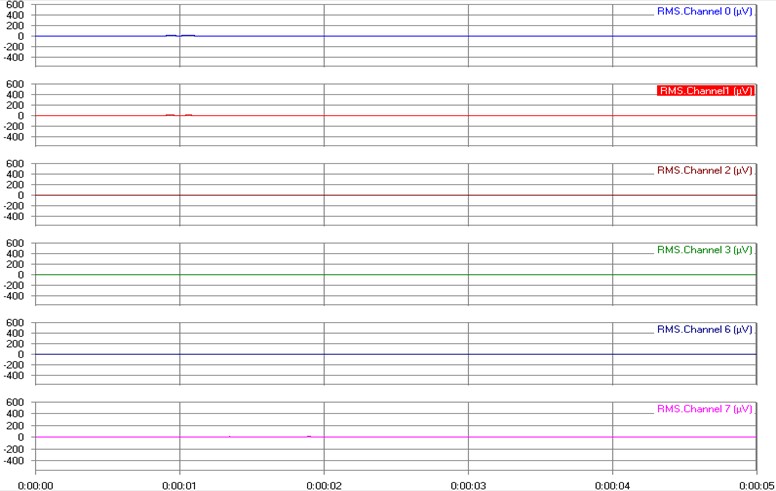
With the FOA in the mouth all measurements improved with a more symmetrical sEMG in T2 in rest and isometric contraction measurements as can be seen in Fig. 1, 2, 3 and 4. The sEMG in rest position showed and improvement as can be seen comparing Fig. 2 and 4. The electrical activity of the left masseter diminish and improve the symmetry of muscle activity with the FOA. Comparing Fig. 1 and 3 and increase in the electric activity of all muscles studied during isometric contraction can be observed. The FOA generates a better muscle function using less energy in mandibular rest position improving resting conditions and greater electric activity in all studied muscles during isometric contraction allowing better food crushing conditions. Results showed that these appliances (SN10), in these mouths, fifteen minutes after installation had changed muscular memory, giving to these muscles conditions to work better, using less energy, muscles bilaterally equilibrated (anterior temporal, masseter, suprahyoid).
The main limitations of this study are the sample (only one patient tested) which means that results have to be carefully analysed and studies with bigger samples are necessary to confirm the results obtained here and this study do not aim to check treatment results nor clinical like reduction overjet or bone remodeling in image exams due to the use of the appliance. It was just studied the masseter, temporal and suprahyoid muscles behavior due to treatment of class II malocclusion with SN10. Another point is that there is no long term measurement to check if this changes are temporary of permanent
4. Discussion
Nalamlian and Thongudomporn [20] found a improvement of muscle activity in class II treatment but using intermaxillary elastics. Based on logical thinking, what very often does not correspond to scientific evidence, it is expected this improvement since Liu et al. [21] reported improvement in the masseter muscle activity in orthodontic class II treatment and, using transcranial magnetic stimulation reported a change in the central nervous system behavior due to the treatment. Besides these findings, the results of this investigation provide data that showed improvement in the stomatognathic muscles. For sure RCT are necessary to check the findings. If the findings of this case report study are confirmed in studies with a bigger sample the sEMG is a very efficient way to check the precision of FOA construction. Another point to be checked is if with other types of FOA results are the same or it can vary with the type of FOA used or even with the type of malocclusion of the individual.
5. Conclusions
The protocol to check the manufacturing of functional orthopedic appliances using surface EMG proved to be valid in this case report study.
Further investigations are needed to confirm this protocol and check if the same happens with other types of functional orthopedics appliances.
References
-
M. R. Xavier Sancho Rios, A. Alves de Carvalho, A. Silveira Martins, A. Souza Nery, and M. A. Drummond, “Jaw functional orthopedics is a therapeutic alternative for class III malocclusion: a case report,” Jaw Functional Orthopedics and Craniofacial Growth, Vol. 1, No. 2, pp. 44–53, Dec. 2021, https://doi.org/10.21595/jfocg.2021.22059
-
F. Monte Callado and M. L. Sperandeo, “Anterior crossbite correction in early mixed dentition stage using functional jaw orthopedics principles: a case report with two-years follow-up,” Jaw Functional Orthopedics and Craniofacial Growth, Vol. 1, No. 2, pp. 62–74, Dec. 2021, https://doi.org/10.21595/jfocg.2021.22173
-
O. Santiago Júnior, “Does Planas’ Equiplan really work in deep bite treatment?,” Jaw Functional Orthopedics and Craniofacial Growth, Vol. 1, No. 2, pp. 75–80, Dec. 2021, https://doi.org/10.21595/jfocg.2021.22329
-
M. T. C. Soares and O. Santiago, “Is jaw functional orthopedics an efficient tool to treat anterior open bite? A retrospective study,” Jaw Functional Orthopedics and Craniofacial Growth, Vol. 2, No. 1, pp. 11–15, Jun. 2022, https://doi.org/10.21595/jfocg.2022.22682
-
M. Bovi Corsi, “Successful balance of occlusal plane using functional orthopedics appliance,” Jaw Functional Orthopedics and Craniofacial Growth, Vol. 2, No. 2, pp. 107–114, Nov. 2022, https://doi.org/10.21595/jfocg.2022.22805
-
R. C. Carneiro Chagas Tanus and O. Santiago, “Behavior of the mandibular length in class II non-growing patients treated with jaw functional orthopedics,” Jaw Functional Orthopedics and Craniofacial Growth, Vol. 2, No. 3, pp. 151–157, Dec. 2022, https://doi.org/10.21595/jfocg.2022.23008
-
V. G. Francisco de Assis, S. Gribel, and A. Mamede, “Anterior crossbite treatment using functional orthopedic appliance: a case report,” Jaw Functional Orthopedics and Craniofacial Growth, Vol. 3, No. 1, pp. 19–31, Jun. 2023, https://doi.org/10.21595/jfocg.2023.23333
-
O. Santiago Júnior, M. V. Lucas Ferreira, and R. Huebner, “Treatment of temporomandibular dysfunction with jaw functional orthopedics: a retrospective study,” Jaw Functional Orthopedics and Craniofacial Growth, Vol. 1, No. 1, pp. 18–27, Jun. 2021, https://doi.org/10.21595/jfocg.2021.22080
-
C. A. O. Machado and P.-C. Simamoto, “Functional orthopedic device type Sn20 – a therapeutic resource in the control of chronic temporomandibular dysfunction – case report,” Jaw Functional Orthopedics and Craniofacial Growth, Vol. 2, No. 2, pp. 115–118, Nov. 2022, https://doi.org/10.21595/jfocg.2022.22868
-
D. A. Lentini-Oliveira, “Planas direct tracks to treat functional crossbites in children: scientific evidence,” Jaw Functional Orthopedics and Craniofacial Growth, Vol. 2, No. 2, pp. 24–31, Nov. 2022, https://doi.org/10.21595/jfocg.2022.22739
-
O. Santiago, “Treatment of vertical problems with jaw functional orthopedics based on scientific evidence. Part 1: anterior open bite,” Jaw Functional Orthopedics and Craniofacial Growth, Vol. 2, No. 2, pp. 41–45, Nov. 2022, https://doi.org/10.21595/jfocg.2022.22778
-
O. Santiago Júnior, “Treatment of vertical problems with jaw functional orthopedics based on scientific evidence. Part 2: deep bite,” Jaw Functional Orthopedics and Craniofacial Growth, Vol. 2, No. 2, pp. 46–49, Nov. 2022, https://doi.org/10.21595/jfocg.2022.22779
-
K. O. ’Brien, “Effectiveness of early orthodontic treatment with the Twin-block appliance: A multicenter, randomized, controlled trial. Part 2: Psychosocial effects,” American Journal of Orthodontics and Dentofacial Orthopedics, Vol. 124, pp. 488–495, 2003.
-
A. Santamaría-Villegas, R. Manrique-Hernandez, E. Alvarez-Varela, and C. Restrepo-Serna, “Effect of removable functional appliances on mandibular length in patients with class II with retrognathism: systematic review and meta-analysis,” BMC Oral Health, Vol. 17, No. 1, p. 52, Feb. 2017, https://doi.org/10.1186/s12903-017-0339-8
-
P. Cozza, T. Baccetti, L. Franchi, L. de Toffol, and J. J. A. Mcnamara, “Mandibular changes produced by functional appliances in Class II malocclusion: A systematic review,” American Journal of Orthodontics and Dentofacial Orthopedics, Vol. 129, 2006.
-
E. Sakai, “Avaliação eletromiográfica de músculos da mastigação em pacientes portadores de maloclusão tratados com Ortopedia Funcional dos Maxilares,” (in Portuguese), Universidade Estadual de Campinas, Piracicaba, SP, 2006.
-
R. E. Moyers, “Temporomandibular muscle contraction patterns in Angle Class II division I malocclusion,” American Journal of Orthodontics, Vol. 35, No. 7, pp. 837–857, 1949.
-
R. E. Moyers, “An electromyographic analysis of certain muscles involved in temporomandibular movement,” American Journal of Orthodontics, Vol. 36, No. 7, pp. 481–515, 1950.
-
W. A. Simões, Ortopedia Funzionale Dei Mascellari Attraverso La Riabilitazione Neuro-Occlusale. Trestina: Nike Srl, 2010.
-
N. Nalamliang and U. Thongudomporn, “Effects of class II intermaxillary elastics on masticatory muscle activity balance, occlusal contact area and masticatory performance: A multicenter randomised controlled trial,” Journal of Oral Rehabilitation, Vol. 50, No. 2, pp. 131–139, Dec. 2022, https://doi.org/10.1111/joor.13395
-
W. Liu, C. Cui, Z. Hu, J. Li, and J. Wang, “Changes of neuroplasticity in cortical motor control of human masseter muscle related to orthodontic treatment,” Journal of Oral Rehabilitation, Vol. 49, No. 2, pp. 258–264, Dec. 2021, https://doi.org/10.1111/joor.13298
About this article

The authors have not disclosed any funding.
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Orlando Santiago Junior – writing review and editing, methodology. Eduardo Sakai – Conceptualiztion, investigation, project administration, writing original draft preparation, methodology. Esther Tamanaga Yamamoto – investigation, data curation. Cintia Aparecida Damos Simões – investigation, data curation. Luciano Wagner Ribeiro – writing original draft preparation, investigation. Jordana Mendonça – investigation, data curation.
The authors declare that they have no conflict of interest.
The investigation was realized under the consent of Ethic Committee of Universidade Federal de Campinas (UNICAMP), Piracicaba, Brazil under protocol 159/2004.
