Abstract
Bruxism is a repetitive jaw-muscle activity characterized by clenching or grinding of the teeth, and it represents a significant clinical challenge in both dentistry and psychiatry. Selective serotonin reuptake inhibitors (SSRIs), the most widely prescribed class of antidepressants worldwide, have been increasingly implicated as a pharmacological trigger for the onset or exacerbation of bruxism. This narrative review synthesizes the available clinical evidence from case reports, case series, and observational studies examining the relationship between SSRI use and bruxism intensity. The putative neurobiological mechanisms linking serotonergic modulation to masticatory motor activity are explored, including the role of serotonin-dopamine interactions in the basal ganglia and the disruption of central pattern generators governing jaw movements during sleep. Current pharmacological management strategies, including the adjunctive use of buspirone, gabapentin, and dose modification, are critically evaluated. The review highlights the need for prospective controlled studies to establish causal relationships, quantify dose-response effects, and develop evidence-based treatment algorithms for SSRI-associated bruxism. In conclusion, although the current evidence is largely derived from case reports and small observational studies, the consistent temporal association between SSRI initiation and bruxism onset, the dose-dependent trend reported in prevalence studies, and the favorable response to adjunctive buspirone collectively support a likely causal role of SSRIs in inducing or intensifying bruxism, and justify routine clinical surveillance for this adverse effect in patients receiving serotonergic antidepressants.
Highlights
- SSRIs can induce or intensify bruxism — predominantly sleep bruxism — typically within the first weeks of thera across case reports, case series, and a systematic review.
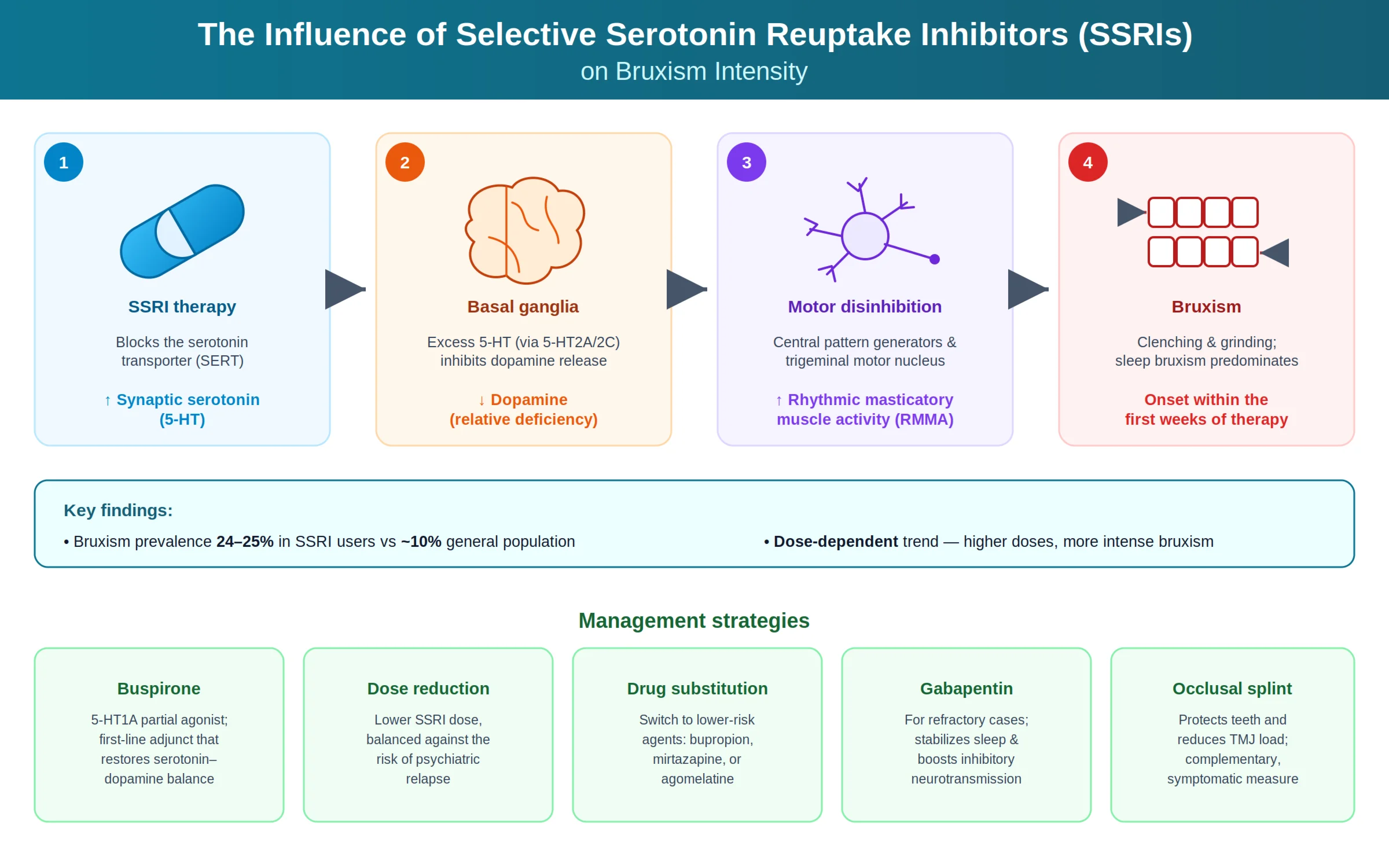
- The principal mechanism is a serotonin–dopamine imbalance: elevated synaptic 5-HT (via 5-HT2A/2C receptors) suppresses dopaminergic transmission in the basal ganglia, disinhibiting central pattern generators and increasing rhythmic masticatory muscle activity.
- Prevalence is markedly higher and dose-dependent in SSRI users (≈24–25%) versus the general population (≈10%), suggesting higher doses are associated with more intense bruxism.
1. Introduction
Bruxism is defined as a repetitive jaw-muscle activity characterized by clenching or grinding of the teeth and/or by bracing or thrusting of the mandible [1]. It is broadly classified into sleep bruxism (SB), which occurs during sleep, and awake bruxism (AB), which manifests during wakefulness. Epidemiological studies suggest that SB affects approximately 8-16 % of the adult population, while AB prevalence ranges from 22-31 % [2]. Bruxism can lead to significant clinical consequences, including dental attrition, temporomandibular joint disorders (TMD), myofascial pain, headaches, and impaired quality of life.
Selective serotonin reuptake inhibitors (SSRIs) are the most commonly prescribed class of antidepressants and are used in the management of major depressive disorder, generalized anxiety disorder, obsessive-compulsive disorder, panic disorder, and post-traumatic stress disorder [3]. Since the seminal case reports by Ellison and Stanziani in 1993 [4], a growing body of evidence has linked SSRI use to the development or worsening of bruxism, particularly sleep bruxism. This association poses a significant clinical dilemma, as the psychiatric conditions treated with SSRIs often coexist with bruxism, and discontinuation of antidepressant therapy may not be feasible.
The objective of this narrative review is to examine the current evidence regarding the influence of SSRIs on bruxism intensity, explore the underlying neurobiological mechanisms, summarize the clinical features and risk factors of SSRI-associated bruxism, and evaluate available management strategies.
2. Pathophysiology of bruxism
2.1. Central mechanisms
Bruxism is now understood to be primarily regulated by central nervous system mechanisms rather than peripheral occlusal factors [5]. Sleep bruxism is classified as a sleep-related movement disorder and is closely associated with micro-arousals during non-REM sleep [6]. The rhythmic masticatory muscle activity (RMMA) observed in SB episodes is generated by central pattern generators in the brainstem, which are modulated by cortical and subcortical inputs [7].
2.2. Role of neurotransmitters
The dopaminergic and serotonergic systems play critical roles in the regulation of motor activity, including the orofacial musculature. Dopamine, acting primarily through D1 and D2 receptors in the basal ganglia, modulates the inhibitory control of motor circuits. Studies using the D2 receptor agonist bromocriptine have shown reductions in SB episodes, supporting the role of the dopaminergic system [8]. Furthermore, pramipexole, another dopamine agonist, has shown efficacy in reducing SB in a randomized crossover study [9].
Serotonin (5-hydroxytryptamine, 5-HT) is a key modulator of mood, sleep architecture, and motor function. The serotonergic raphe nuclei project widely to cortical, limbic, and motor areas. Importantly, serotonin exerts an inhibitory influence on dopaminergic neurons in the mesocortical and nigrostriatal pathways. SSRIs, by blocking the serotonin transporter (SERT) and increasing synaptic 5-HT concentrations, may secondarily suppress dopaminergic transmission in the basal ganglia, thereby disinhibiting motor circuits and facilitating bruxism [10]. This serotonin-dopamine interaction is considered the principal neurobiological mechanism underlying SSRI-induced bruxism [11].
3. Clinical evidence: SSRIs and bruxism
3.1. Case reports and case series
The earliest and most frequently cited evidence linking SSRIs to bruxism comes from case reports and case series. Ellison and Stanziani [4] described four patients who developed nocturnal bruxism within 3-4 weeks of initiating fluoxetine or sertraline therapy. Symptoms were characterized by tooth grinding, jaw pain upon awakening, and reports of grinding sounds by bed partners. In all cases, bruxism resolved upon drug discontinuation or addition of buspirone.
Wise [12] reported a case of citalopram-induced nocturnal bruxism with an onset of approximately two weeks after drug initiation. Milanlioglu [13] documented severe paroxetine-induced sleep bruxism that was successfully treated with buspirone 10 mg/day. Kuloglu et al. [14] reported three cases of venlafaxine-associated nocturnal bruxism (venlafaxine, an SNRI, shares the serotonergic mechanism), with symptom onset within 1-3 weeks. These reports consistently indicate a temporal relationship between SSRI initiation and bruxism onset, with resolution upon dose reduction, drug discontinuation, or the addition of adjunctive agents.
3.2. Systematic review evidence
Garrett and Hawley [15] conducted a systematic review of published case reports of SSRI-associated bruxism. Their analysis identified reports involving fluoxetine, sertraline, paroxetine, citalopram, escitalopram, and fluvoxamine, as well as SNRIs such as venlafaxine and duloxetine. The review found that sleep bruxism was the most commonly reported subtype, onset typically occurred within the first few weeks of treatment, and the most frequently employed management strategy was the addition of buspirone (a 5-HT1A partial agonist). The authors concluded that while the evidence is limited to case-level data, the consistent temporal associations and the pharmacological plausibility of the serotonin-dopamine mechanism strongly support a causal relationship.
3.3. Prevalence studies
Uca et al. [16] conducted a cross-sectional study investigating the prevalence of bruxism among patients receiving antidepressant therapy. Their findings indicated that patients on SSRIs had a significantly higher prevalence of bruxism compared to controls, with reported rates ranging from 24-25 % among SSRI users versus approximately 10 % in the general population. Importantly, the study also found a dose-dependent trend, suggesting that higher SSRI doses may be associated with more intense bruxism, though this finding requires confirmation in larger prospective studies.
4. Proposed mechanisms of SSRI-induced bruxism
4.1. Serotonin-dopamine imbalance
The most widely accepted mechanism for SSRI-induced bruxism involves the indirect suppression of dopaminergic neurotransmission via elevated serotonin levels. SSRIs increase synaptic 5-HT concentrations by blocking the serotonin transporter. The excess serotonin, acting through 5-HT2A and 5-HT2C receptors on dopaminergic neurons, exerts an inhibitory effect on dopamine release in the mesocortical and nigrostriatal pathways [10]. The resulting relative dopamine deficiency in the basal ganglia may disinhibit the trigeminal motor nucleus and central pattern generators, leading to increased rhythmic masticatory muscle activity and bruxism [17].
4.2. Effects on sleep architecture
SSRIs are known to alter sleep architecture, including suppression of REM sleep, increased sleep latency, and fragmentation of non-REM sleep with increased micro-arousals [18]. Since SB episodes are predominantly associated with micro-arousals during non-REM sleep transitions [6], SSRI-induced sleep fragmentation may represent an additional mechanism by which these drugs promote or intensify bruxism. The relationship between SSRI-induced sleep disruption and SB intensity warrants further investigation with polysomnographic studies.
4.3. 5-HT1A receptor involvement
The efficacy of buspirone, a 5-HT1A partial agonist, in managing SSRI-induced bruxism provides indirect evidence for the involvement of serotonin receptor subtypes in the pathogenesis of this adverse effect. The 5-HT1A receptor acts as both a presynaptic autoreceptor (reducing serotonin release) and a postsynaptic receptor modulating dopaminergic function. By activating presynaptic 5-HT1A autoreceptors, buspirone may reduce the excessive serotonergic tone induced by SSRIs, thereby restoring the serotonin–dopamine balance in motor circuits [19].
5. Management strategies
5.1. Dose reduction and drug substitution
When SSRI-associated bruxism is suspected, the initial approach should include a careful assessment of the temporal relationship between drug initiation (or dose escalation) and bruxism onset. Dose reduction may alleviate symptoms in some patients, though this must be balanced against the risk of psychiatric relapse [11]. Drug substitution to an antidepressant with a different mechanism of action (e.g., bupropion, mirtazapine, or agomelatine) may be considered, as these agents have not been consistently linked to bruxism and may in fact have a lower risk profile [17].
5.2. Buspirone
Buspirone, a 5-HT1A partial agonist, is the most frequently cited pharmacological antidote for SSRI-induced bruxism. Bostwick and Jaffee [20] first reported its efficacy in four patients with SSRI-associated bruxism at doses of 5-10 mg twice daily. Subsequent case reports have confirmed these findings [21]. Buspirone is hypothesized to counteract the excessive serotonergic stimulation by activating presynaptic 5-HT1A autoreceptors, thereby reducing serotonin release and partially restoring dopaminergic function in motor circuits. A recent systematic review by Chouinard et al. [19] supports the use of buspirone as a first-line adjunctive treatment for SSRI-induced bruxism.
5.3. Gabapentin
Gabapentin, a GABA analogue that modulates calcium channels and increases GABAergic inhibition, has been reported to alleviate SSRI-induced bruxism in isolated case reports. Soyata and Oflaz [22] described a patient with SSRI-induced sleep bruxism that was refractory to dose reduction but responded to gabapentin 300 mg at bedtime. Gabapentin’s mechanism in bruxism may involve stabilization of sleep architecture and enhancement of inhibitory neurotransmission in the central motor circuits. However, evidence remains limited to case-level data.
5.4. Intra-oral devices and non-pharmacological approaches
Intra-oral devices remain a cornerstone of symptomatic management for bruxism, regardless of etiology. While they do not address the underlying cause, they protect dental surfaces from attrition, reduce TMJ loading, and may decrease masticatory muscle hyperactivity. In the context of SSRI-induced bruxism, splints should be used as a complementary measure while pharmacological strategies are optimized [7].
6. Discussion
The evidence linking SSRIs to bruxism, while predominantly derived from case reports and case series, is consistent and pharmacologically plausible. The temporal relationship between SSRI initiation and bruxism onset, the dose-dependent trend observed in some studies, the resolution of symptoms upon drug discontinuation, and the response to pharmacological antidotes such as buspirone all support a causal association [15].
However, several limitations must be acknowledged. First, the vast majority of evidence is based on case reports and retrospective studies, which are subject to reporting bias and confounding. The psychiatric conditions for which SSRIs are prescribed (depression, anxiety) are themselves associated with bruxism [23], making it difficult to disentangle the contribution of the drug from that of the underlying disease. Second, objective measurement of bruxism intensity – ideally through polysomnography with electromyographic (EMG) recording – has rarely been employed in published studies; most reports rely on self-reported symptoms or clinical examination findings.
Future research should prioritize prospective, randomized controlled studies comparing bruxism intensity (measured by polysomnography and ambulatory EMG) before and after SSRI initiation, controlling for psychiatric comorbidities. Dose-response studies are needed to determine whether specific SSRI agents or dosage thresholds confer a differential risk of bruxism. Additionally, head-to-head comparisons between different management strategies (buspirone, gabapentin, dose reduction, and drug substitution) in randomized controlled designs would provide the evidence base needed to develop clinical guidelines.
7. Conclusions
The current evidence strongly suggests that SSRIs can induce or exacerbate bruxism, with sleep bruxism being the most commonly reported subtype. The predominant mechanism involves serotonin-mediated suppression of dopaminergic function in the basal ganglia, leading to disinhibition of central pattern generators governing masticatory motor activity. Clinicians prescribing SSRIs should be aware of this adverse effect and should routinely inquire about bruxism-related symptoms. When SSRI-induced bruxism is identified, a stepwise approach involving dose adjustment, the addition of buspirone, or substitution with alternative antidepressants is recommended. Prospective controlled studies are urgently needed to quantify the prevalence, dose-response relationship, and optimal management of this clinically significant drug-induced movement disorder.
References
-
F. Lobbezoo et al., “International consensus on the assessment of bruxism: report of a work in progress,” Journal of Oral Rehabilitation, Vol. 45, No. 11, pp. 837–844, 2018, https://doi.org/10.1111/joor.12663
-
D. Manfredini, E. Winocur, L. Guarda-Nardini, D. Paesani, and F. Lobbezoo, “Epidemiology of bruxism in adults: a systematic review of the literature,” Journal of Orofacial Pain, Vol. 27, No. 2, pp. 99–110, 2013, https://doi.org/10.11607/jop.921
-
A. Cipriani et al., “Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis,” The Lancet, Vol. 391, No. 10128, pp. 1357–1366, 2018, https://doi.org/10.1016/s0140-6736(17)32802-7
-
J. M. Ellison and P. Stanziani, “SSRI-associated nocturnal bruxism in four patients,” The Journal of Clinical Psychiatry, Vol. 54, No. 11, pp. 432–434, 1993.
-
F. Lobbezoo and M. Naeije, “Bruxism is mainly regulated centrally, not peripherally,” Journal of Oral Rehabilitation, Vol. 28, No. 12, pp. 1085–1091, 2001, https://doi.org/10.1046/j.1365-2842.2001.00839.x
-
G. M. Macaluso, P. Guerra, G. Di Giovanni, M. Boselli, L. Parrino, and M. G. Terzano, “Sleep bruxism is a disorder related to periodic arousals during sleep,” Journal of Dental Research, Vol. 77, No. 4, pp. 565–573, 1998, https://doi.org/10.1177/00220345980770040901
-
G. J. Lavigne, S. Khoury, S. Abe, T. Yamaguchi, and K. Raphael, “Bruxism physiology and pathology: an overview for clinicians,” Journal of Oral Rehabilitation, Vol. 35, No. 7, pp. 476–494, 2008, https://doi.org/10.1111/j.1365-2842.2008.01881.x
-
F. Lobbezoo, J.-P. Soucy, N. G. Hartman, J. Y. Montplaisir, and G. J. Lavigne, “Effects of the D2 receptor agonist bromocriptine on sleep bruxism: report of two single-patient clinical trials,” Journal of Dental Research, Vol. 76, No. 9, pp. 1610–1614, 1997, https://doi.org/10.1177/00220345970760091401
-
B. J. Cahlin, J. Hedner, and L. Dahlström, “A randomized, open-label, crossover study of the dopamine agonist, pramipexole, in patients with sleep bruxism,” Journal of Sleep Research, Vol. 26, No. 1, pp. 64–72, 2016, https://doi.org/10.1111/jsr.12440
-
G. Falisi, C. Rastelli, F. Panti, H. Maglione, and R. Quezada Arcega, “Psychotropic drugs and bruxism,” Expert Opinion on Drug Safety, Vol. 13, No. 10, pp. 1319–1326, 2014, https://doi.org/10.1517/14740338.2014.947262
-
R. Rajan and Y.-M. Sun, “Reevaluating antidepressant selection in patients with bruxism and temporomandibular joint disorder,” Journal of Psychiatric Practice, Vol. 23, No. 3, pp. 173–179, 2017, https://doi.org/10.1097/pra.0000000000000227
-
Wise and M. E. J., “Citalopram-induced bruxism,” British Journal of Psychiatry, Vol. 178, No. 2, pp. 182–182, 2018, https://doi.org/10.1192/bjp.178.2.182
-
A. Milanlıoglu, “Paroxetine-induced severe sleep bruxism successfully treated with buspirone,” Clinics, Vol. 67, No. 2, pp. 191–192, 2012, https://doi.org/10.6061/clinics/2012(02)17
-
M. Kuloglu, O. Ekinci, and A. Caykoylu, “Venlafaxine-associated nocturnal bruxism in a depressive patient successfully treated with buspirone,” Journal of Psychopharmacology, Vol. 24, No. 4, pp. 627–628, Mar. 2009, https://doi.org/10.1177/0269881109102612
-
A. R. Garrett and J. S. Hawley, “Ssri-associated bruxism: A systematic review of published case reports,” Neurology Clinical Practice, Vol. 8, No. 2, pp. 135–141, 2018, https://doi.org/10.1212/cpj.0000000000000433
-
A. U. Uca et al., “Antidepressant-induced sleep bruxism,” Clinical Neuropharmacology, Vol. 38, No. 6, pp. 227–230, 2015, https://doi.org/10.1097/wnf.0000000000000108
-
E. Winocur, A. Gavish, M. Voikovitch, A. Emodi-Perlman, and I. Eli, “Drugs and bruxism: a critical review,” Journal of Orofacial Pain, Vol. 17, No. 2, pp. 99–111, 2003.
-
P. Mayer, R. Heinzer, and G. Lavigne, “Sleep bruxism in respiratory medicine practice,” Chest, Vol. 149, No. 1, pp. 262–271, Jan. 2016, https://doi.org/10.1378/chest.15-0822
-
C. de Baat et al., “Medications and addictive substances potentially inducing or attenuating sleep bruxism and/or awake bruxism,” Journal of Oral Rehabilitation, Vol. 48, No. 3, pp. 343–354, 2020, https://doi.org/10.1111/joor.13061
-
J. M. Bostwick and M. S. Jaffee, “Buspirone as an antidote to SSRI-induced bruxism in 4 cases,” The Journal of Clinical Psychiatry, Vol. 60, No. 12, pp. 857–860, 1999, https://doi.org/10.4088/jcp.v60n1209
-
R. Çolak Sivri and F. Akça, “Buspirone in the treatment of fluoxetine-induced sleep bruxism,” Journal of Child and Adolescent Psychopharmacology, Vol. 26, No. 8, pp. 762–763, 2016, https://doi.org/10.1089/cap.2016.0075
-
A. Z. Soyata and S. Oflaz, “Gabapentin treatment in bruxism associated with fluoxetine,” Journal of Clinical Psychopharmacology, Vol. 35, No. 4, pp. 481–483, 2015, https://doi.org/10.1097/jcp.0000000000000337
-
G. Fernandes, A. L. Franco-Micheloni, J. T. T. Siqueira, D. A. G. Gonçalves, and C. M. Camparis, “Parafunctional habits are associated cumulatively to painful temporomandibular disorders in adolescents,” Brazilian Oral Research, Vol. 30, No. 1, pp. e15–e15, 2016, https://doi.org/10.1590/1807-3107bor-2016.vol30.0015
About this article

The authors have not disclosed any funding.
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Dr. Patricia Valério is an editorial board member for Jaw Functional Orthopedics and Craniofacial Growth and was not involved in the editorial review and/or the decision to publish this article.
