Abstract
This study aimed to evaluate whether inter-arch space, expressed as oral cavity volume, increases following malocclusion treatment. A retrospective analysis was conducted on 10 patients (aged 6-28 years) with mixed and permanent dentitions presenting different types of malocclusion. All patients underwent treatment involving transverse and/or sagittal expansion, mandibular posture modification, and occlusal harmonization using Jaw Functional Orthopedics appliances. Inter-arch volume was assessed using dental casts obtained before and after treatment. A standardized acrylic resin filling technique was applied to delimit the intraoral space, and volume measurements were obtained using the fluid displacement method based on Archimedes’ principle. All patients showed an increase in inter-arch volume after treatment, with a mean increase of 30.4 % (range: 14.28 %-4.54 %). The mean volume increased from 16.8 mL pre-treatment to 21.9 mL post-treatment, corresponding to an average gain of 5.1 mL. These findings suggest that malocclusion treatment using Jaw Functional Orthopedics may increase intraoral space, potentially improving conditions for dental alignment and tongue posture. Further studies with larger samples and controlled designs are required to confirm these results.
Highlights
- This pilot study introduces an objective and reproducible method for quantifying functional inter-arch space following Jaw Functional Orthopedics.
- Inter-arch volume increased in all patients following Jaw Functional Orthopedics treatment.
- Mean inter-arch volume increased by 30.4% after treatment.
- Inter-arch volume was quantified using Archimedes' fluid displacement principle.
- Increased inter-arch space may improve conditions for dental alignment and tongue posture.
1. Introduction
The volume of the oral cavity corresponds to the space between the maxillary and mandibular arches, where the tongue is positioned and performs its functions. Previous studies have demonstrated a relationship between jaw development and changes in stomatognathic system functions, which may impact overall health and quality of life [1-5].
Understanding craniofacial growth and development is essential for accurate diagnosis, treatment planning, and post-treatment evaluation in orthodontic and orthopedic cases [6]. It is also important to consider the synchronism and synergy among breathing, sucking, and swallowing functions. Disruption of any of these three coordinated and interdependent processes may adversely affect the others [1].
When dental arches are reduced in size and/or poorly related, the available space for proper tongue posture may be compromised. This can result in posterior tongue displacement, reducing the airway space and potentially affecting mastication due to occlusal issues [7, 8], as well as impairing breathing [9].
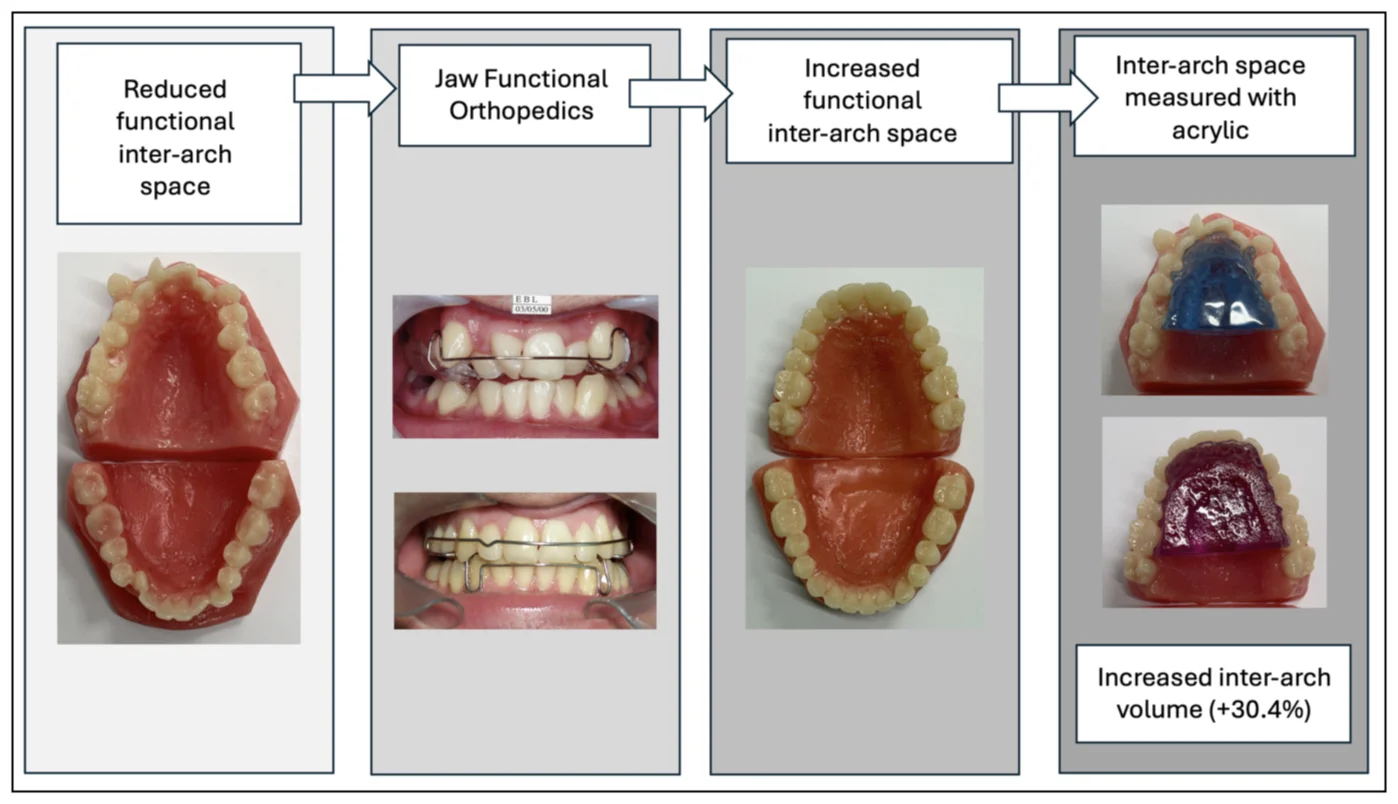
Jaw Functional Orthopedics (JFO) appliances can promote maxillary expansion and induce changes in mandibular position, acting in three dimensions – sagittal, vertical, and transverse – with the aim of achieving harmony between the jaws. This therapeutic approach creates space for proper tooth alignment and tongue positioning, contributing to improved upper airway conditions and restoration of stomatognathic system functions [1, 9-11].
2. Objective
To evaluate whether the inter-arch space increases after malocclusion treatment involving transverse and/or sagittal expansion, changes in mandibular posture, and occlusal harmonization.
3. Methodology
Ten clinical cases (7 females and 3 males) with mixed and permanent dentitions were analyzed. Two cases presented mixed dentition (ages 7 years 6 months and 10 years 10 months; mean age: 8 years 8 months), while eight cases had permanent dentition (ages 14-28 years; mean age: 18 years 2 months). All patients presented malocclusions requiring transverse and/or sagittal dental arch expansion, mandibular posture adjustment, and occlusal harmonization as part of the treatment plan.
3.1. Volume measurement protocol
For each patient, pre-treatment and post-treatment dental casts were prepared (Fig. 1). The models were obtained from alginate impressions (Hidrogum, Zhermack) and poured with orthodontic plaster. All procedures were performed by the same operator to ensure standardization.
The internal volume between the dental arches was quantified using an acrylic resin filling technique developed by the author.
Fig. 1Working models of one of the patients who were involved in the study

a) Before treatment

b) After treatment
The limits for volume measurement were defined as follows:
1) Posterior limit: distal surface of the upper first molars (Figs. 1(a) and 1(b)).
2) Superior limit: palatal vault.
3) Inferior limit: floor of the mouth, defined as 3 mm below the free gingival margin (Fig. 2).
The floor of the mouth region was filled with plaster up to 3 mm below the lingual gingival margin. The space was then sealed with utility wax and internally insulated (Fig. 3(a)).
Acrylic resin was subsequently introduced into the internal space, filling it up to the distal limit of the upper first molars (illustrated in Figs. 2-3). After polymerization, the resin block was removed from the model (Fig. 4).
Volume was measured based on Archimedes’ principle, in which the volume of displaced water corresponds to the volume of the object [12]. Measurements were performed using Becker-type volumetric containers (flat-bottom, wide opening) and a measuring syringe (Fig. 5). All readings were recorded in milliliters using a standardized technique.
The change in volume was defined as the difference between post-treatment and pre-treatment measurements.
Fig. 2Measuring and limiting the lower part: 3 mm below the free marginal gingiva of the premolars


Fig. 3a) Articulated models; b) wax used to seal the resin exit; c) resin inserted into the previously isolated and hydrated model

a)

b)

c)
Fig. 4Polymerized resins, in blue before treatment and in lilac, after treatment



3.2. Study design and treatment
3.2.1. Study design and treatment
This pilot study consisted of a retrospective and descriptive analysis of measurements obtained before and after treatment. No control group was included, and there was no standardization regarding patient age or treatment protocol.
The two patients with Class I malocclusion were treated with a Mauricio expander for 6 months, followed by Indirect Planas Tracks for 1.5 years.
Among the two patients with Class III malocclusion, one patient used a Mauricio-designed appliance with posteroanterior action for the anterior maxilla for 4 months. Both patients were additionally treated with a Mauricio expander for 6 months and the SN3 appliance for 1 year.
The six patients with Class II malocclusion were treated with a Mauricio expander for an average of 7 months. Subsequently, two patients used a Klammt appliance for 1 year, while four patients were treated with Simões Network 1 (SN1) for 1.5 years.
One patient also used a Mauricio distalizer for 4 months to achieve dental arch symmetry and create space for the upper right canine.
Fig. 5Becker and syringe used to measure the resin volume

3.2.2. Ethical aspects
Number of the substantiated opinion of the Research Ethics Committee: 4.390.918.
Number of CAAE: 36113820.7.0000.5102.
4. Results
All cases demonstrated an increase in volume after treatment, with gains ranging from 14.28 % to 54.54 %. Variations in treatment approaches—such as transverse expansion alone, mandibular advancement, and/or increases in vertical dimension—contributed to differences in the magnitude of volume increase.
Table 1 presents the pre- and post-treatment volumes, along with the corresponding percentage increases for all 10 patients.
Table 1Initial and final volumes (mL) and percentage increases by patient
Patient | Age (years) | Sex | Class | Volume Pre (ml) | Volume post (ml) | Increase (%) |
1 | 14 | F | II | 16.0 | 21.5 | 28.00 % |
2 | 16 | F | II | 18.0 | 22.5 | 25.00 % |
3 | 20,5 | F | III | 19.0 | 23.5 | 23.68 % |
4 | 7,5 | F | III | 11.0 | 17.0 | 54.54 % |
5 | 15 | F | II | 17.0 | 23.5 | 38.23 % |
6 | 10 | M | II | 14.0 | 16.0 | 14.28 % |
7 | 18 | F | II | 17.0 | 21.0 | 23.52 % |
8 | 14 | F | II | 16.0 | 21.0 | 31.25 % |
9 | 28 | M | I | 20.0 | 23.5 | 17.50 % |
10 | 22 | M | II | 20.0 | 29.0 | 45.00 % |
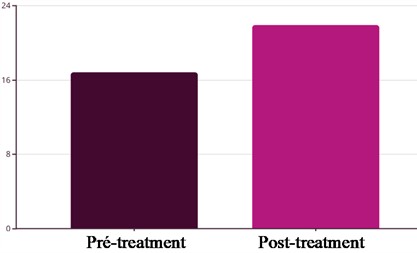
Fig. 6 shows a mean increase of 30.4 % in oral cavity volume after treatment, with a 95 % confidence interval. The mean pre-treatment volume was 16.8 mL, while the mean post-treatment volume was 21.9 mL, resulting in an average absolute increase of 5.1 mL.
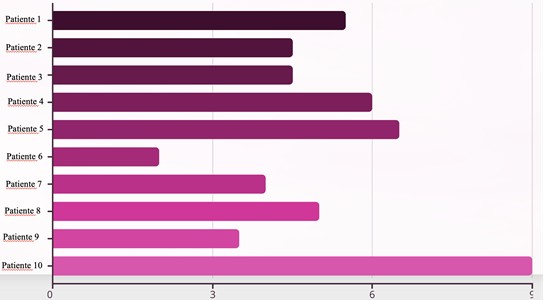
Fig. 7 illustrates the individual variation in volume changes across patients.
Fig. 6Statistical analysis reveals a mean increase of 30.4 % in oral volume after treatment, with a 95 % confidence interval
Statistical insights:
1) Mean pre-treatment volume: 16.8 ml.
2) Mean post-treatment volume: 21.9 ml.
3) Absolute difference: 5.1 ml.
4) Clinical significance confirmed.
Fig. 7Analysis of individual variation by patient: Patient 10 presented the greatest absolute volumetric gain, Patient 6 had the smallest increment observed in the study, average variation among all patients evaluated
5. Discussion
This retrospective exploratory case series analyzed a heterogeneous sample of children, adolescents, and adults undergoing treatment involving transverse and/or sagittal arch expansion, mandibular posture modification, and occlusal harmonization. All cases demonstrated an increase in dental arch space and in the inter-arch oral cavity volume following treatment.
The observed improvements in spatial dimensions and arch morphology are consistent with the clinical objectives of Jaw Functional Orthopedics and with the concept that occlusal balance contributes to the proper functioning of the stomatognathic system and overall quality of life [1, 7-11].
The increase in arch dimensions and volume suggests the potential for space gain through bone remodeling not only in growing patients but also in adults. However, this interpretation should be approached with caution due to the study’s limitations. These include the small sample size ( 10), the heterogeneity of malocclusion types and treatment protocols, and the absence of a control group.
The literature reviewed predominantly reports linear measurements of dental arch changes [13]. To the best of our knowledge, no previous studies have evaluated volumetric changes in the space between dental arches using a comparable methodology.
Future studies should include larger samples and, ideally, randomized controlled trial designs to better isolate the effects of specific interventions on inter-arch volume and tongue space.
6. Conclusions
The findings of this study suggest that treatment guided by the principles of Jaw Functional Orthopedics may increase intraoral space, thereby facilitating proper tooth positioning in both growing patients and adults.
However, randomized controlled clinical trials with improved and standardized measurement protocols are necessary to confirm these findings and strengthen the evidence base.
References
-
W. A. Simões, P. Valério, and D. Duarte, Functional Orthopedics of the Jaws: Research and Clinical Excellence. Nova Odessa, SP: Editora Napoleão Ltda, 2020, pp. 975–85.
-
P. Festa et al., “Association between upper airway obstruction and malocclusion in mouth-breathing children,” Acta Otorhinolaryngologica Italica, Vol. 41, No. 5, pp. 436–442, Oct. 2021, https://doi.org/10.14639/0392-100x-n1225
-
L. Lin, T. Zhao, D. Qin, F. Hua, and H. He, “The impact of mouth breathing on dentofacial development: a concise review,” Frontiers in Public Health, Vol. 10, p. 929165, Sep. 2022, https://doi.org/10.3389/fpubh.2022.929165
-
J. L. Yu, A. Tangutur, E. Thuler, M. Evans, and R. C. Dedhia, “The role of craniofacial maldevelopment in the modern OSA epidemic: a scoping review,” Journal of Clinical Sleep Medicine, Vol. 18, No. 4, pp. 1187–1202, 2022, https://doi.org/10.5664/jcsm.9866
-
G. L. Granja et al., “Predictors associated with malocclusion in children with and without sleep disorders: a cross-sectional study,” Brazilian Oral Research, Vol. 37, p. e106, Oct. 2023, https://doi.org/10.1590/1807-3107bor-2023.vol37.0106
-
S. A. Hallett, W. Ono, R. T. Franceschi, and N. Ono, “Cranial base synchondrosis: chondrocytes at the hub,” International Journal of Molecular Sciences, Vol. 23, No. 14, p. 7817, Jul. 2022, https://doi.org/10.3390/ijms23147817
-
A. Hamdi, R. Kallala, and B. Harzallah, “Chewing efficiency and contact area discrepancies in Angle’s class I and II malocclusion: a comparative study,” The Saudi Dental Journal, Vol. 36, No. 4, pp. 633–637, Apr. 2024, https://doi.org/10.1016/j.sdentj.2023.12.016
-
K. S. R. Au Yeung, Z. Shan, F. H. K. M. H. Sum, K. W. F. Wong, H. M. G. Lee, and Y. Yang, “Association between occlusal features and masticatory function in Hong Kong preschool children: a survey with one-year longitudinal follow-up,” BMC Oral Health, Vol. 24, No. 1, p. 187, Feb. 2024, https://doi.org/10.1186/s12903-024-03895-6
-
R. Bernardes, L. M. Di Bisceglie Ferreira, A. J. Machado Júnior, and M. H. Jones, “Effectiveness of functional orthopedic appliances as an alternative treatment among children and adolescents with obstructive sleep apnea: systematic review and meta-analysis,” Sleep Medicine, Vol. 105, pp. 88–102, May 2023, https://doi.org/10.1016/j.sleep.2023.03.008
-
E. Cesur, S. Bayrak, E. Kursun-Çakmak, C. Arslan, A. Köklü, and K. Orhan, “Evaluating the effects of functional orthodontic treatment on mandibular osseous structure using fractal dimension analysis of dental panoramic radiographs,” The Angle Orthodontist, Vol. 90, No. 6, pp. 783–793, Nov. 2020, https://doi.org/10.2319/012020-39.1
-
S. Ashok et al., “An assessment of masticatory efficiency and occlusal load distribution in adolescent patients undergoing orthodontic treatment with functional jaw orthopedics: a prospective cohort study,” Journal of Stomatology, Oral and Maxillofacial Surgery, Vol. 124, No. 6, p. 101570, Dec. 2023, https://doi.org/10.1016/j.jormas.2023.101570
-
“The Ten Books on Architecture.” https://math.nyu.edu/archimedes/crown/vitruvius.html
-
A. Aliaga-Del Castillo et al., “Dental arch changes after open bite treatment with spurs associated with posterior build-ups in the mixed dentition: a randomized clinical trial,” American Journal of Orthodontics and Dentofacial Orthopedics, Vol. 159, No. 6, pp. 714–723.e1, Jun. 2021, https://doi.org/10.1016/j.ajodo.2020.11.036
About this article

The authors have not disclosed any funding.
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
The authors declare that they have no conflict of interest.
Number of the substantiated opinion of the Research Ethics Committee: 4.390.918.
Number of CAAE: 36113820.7.0000.5102.
