Abstract
The objective was to compare postural alignment and balance-related outcomes between women with generalized joint hypermobility (GJH) and their non-hypermobile counterparts. Materials and Methods: Seventy-six young women, aged 21.32 (1.34) years on average, were enrolled. Thirty-nine participants met the criteria for GJH, whereas 37 women without GJH formed the control group. Body posture was evaluated with the Diers Formetric 4D system. The following posture parameters were selected for analysis: sagittal imbalance, thoracic kyphosis angle, lumbar lordosis angle, pelvic torsion, pelvic rotation, vertebral rotation. Balance performance was measured with the Biodex Balance System SD using the Modified Clinical Test of Sensory Integration and Balance test. Results and conclusions: Most postural parameters did not differ significantly between women with and without GJH, including sagittal imbalance, thoracic kyphosis angle, lumbar lordosis angle, pelvic rotation in the horizontal plane, and vertebral rotation. However, women with GJH demonstrated a significantly greater pelvic torsion angle in the sagittal plane. In addition, static balance was significantly poorer in women with GJH compared with the control group. These findings suggest that GJH is not associated with major differences in most spinal and pelvic posture parameters, but may be related to increased sagittal pelvic torsion and impaired static balance.
Highlights
- Women with generalized joint hypermobility demonstrated poorer static balance than non-hypermobile women.
- Most spinal and pelvic posture parameters were similar between women with and without generalized joint hypermobility.
- Women with generalized joint hypermobility showed greater sagittal-plane pelvic torsion than non-hypermobile women.
1. Introduction
Generalized joint hypermobility (GJH) refers to excessive mobility across several joints, affecting both the appendicular joints of the upper and lower limbs and the axial skeleton. It may be symptomatic or asymptomatic, and these terms are often described synonymously in the scientific literature as syndromic and non-syndromic generalized GJH [1, 2].
Scientists suggest that the development of GJH is influenced by genetic factors, as this condition is most inherited in an autosomal dominant manner and may be associated with genes encoding structural connective tissue proteins [3]. The reported prevalence of GJH in children, adolescents, and young adults varies between 12 % and 28 %, and the condition appears to be more frequent among children and females [4].
In asymptomatic cases of GJH, no clinical musculoskeletal symptoms are observed, however, individuals with this characteristic may require preventive measures, such as regular physical activity or appropriate ergonomics, in order to avoid potential musculoskeletal disorders in the future [1]. Meanwhile, individuals with symptomatic GJH exhibit various clinical signs related to the musculoskeletal system or skin changes, which are also common in individuals with hypermobility spectrum disorders or hypermobile Ehlers-Danlos syndrome. These signs include recurrent back or joint pain, joint dislocations occurring more than once, increased skin elasticity, and others [1, 5]. Symptomatic GJH has been reported to affect approximately 0.5 %-2 % of the general population [6].
The assessment of GJH in clinical practice is highly significant, as it is often considered a primary diagnostic criterion for inherited connective tissue disorders. Although GJH may also be present in individuals without any symptoms, studies demonstrate its associations with various health disorders [6, 8]. Therefore, early identification is important, especially in individuals experiencing pain without clear degenerative or inflammatory joint changes, as unrecognized symptoms of GJH may be misattributed to other pathological conditions, increasing the likelihood of inappropriate treatment or unnecessary interventions [9, 10].
Individuals with confirmed GJH often experience various musculoskeletal problems. These may arise due to increased elasticity of tissues that are sensitive to mechanical forces such as gravity, physical activity, and body weight. During periods of physiological growth and maturation, this may lead to the development of certain postural characteristics or musculoskeletal pathologies [2]. Because joints with increased range of motion are unstable, the body activates surrounding muscles to stabilize them, and due to their constant load, muscle tension, spasms, inflammation, or pain may occur [13]. GJH may lead to postural changes over time, such as scoliosis, increased thoracic kyphosis and lordosis, flat feet, and hallux valgus deformity [2, 15].
These individuals often exhibit decreased muscle strength and impaired proprioception, making it difficult to perceive body position in space, and the body gradually adapts to incorrect posture. This may manifest as a tendency to sit in a slouched position with posterior pelvic tilt, further promoting the development of poor posture [16].
Studies analyzing the relationship between GJH and the musculoskeletal system often find significant associations: GJH may be a risk factor for spinal deformities such as idiopathic scoliosis or increased thoracic kyphosis [17].
One of the most important abilities ensuring stable movement is proprioception, which helps individuals perceive both static and dynamic orientation in space [18]. Proprioceptive impairments, leading to activity limitations and reduced participation in daily activities, are common in individuals with GJH [19]. These changes may increase the risk of musculoskeletal injuries and are evident when testing joints that often exhibit increased range of motion [20]. Due to altered proprioception, individuals with GJH often experience difficulties performing tasks requiring balance, and the body activates additional muscles to maintain stability [21]. Other studies indicate that these individuals may be more prone to recurrent microtrauma, and signs such as increased postural sway at rest, slower walking speed, shorter step length, and longer stance phase duration may indicate impaired balance [22, 23].
Considering the potential differences in body posture and balance among individuals with GJH, it is important to examine these factors in order to better understand their possible impact on musculoskeletal health. We investigated whether postural alignment and balance performance differed between women presenting with GJH and non-hypermobile women.
2. Materials and methods
2.1. Participants
Data collection took place in March 2026 at the Department of Sports Medicine of the Lithuanian University of Health Sciences. The study protocol was approved by the Bioethics Center of the Lithuanian University of Health Sciences (No. 2026-BEC2-0204). Seventy-six young women were included in the study, with a mean age of 21.32±1.34 years. Eligibility was restricted to women aged 20-25 years who reported low or moderate physical activity and agreed to participate voluntarily. The exclusion criteria included pregnancy, diagnosed connective tissue disorders, and involvement in elite or high-performance sport. According to GJH status, participants were assigned to the hypermobility group ( 39) or the control group without GJH ( 37). Participants who scored 5 or more points on the Beighton scale were assigned to the study group, while participants who scored 4 or fewer points were assigned to the control group. The two groups did not differ significantly in age ( 791.5; 0.450). The overall mean BMI of the participants was 22.57 (SD = 2.32), and BMI did not differ significantly between the groups ( –1.594; 0.115). Physical activity levels, assessed using the International Physical Activity Questionnaire-Short Form, were comparable between the GJH and control groups ( 0.000; 1.000).
2.2. Methods
Generalized joint hypermobility (GJH) was assessed using the Beighton score. During the assessment of GJH using the Beighton score the range of motion of five joint movements was evaluated, four of which were assessed bilaterally: extension of the fifth finger beyond 90 degrees in both hands, passive apposition of both thumbs to the forearm, elbow hyperextension greater than 10 degrees in both arms, knee hyperextension greater than 10 degrees in both legs, and forward trunk flexion with both palms placed flat on the floor while keeping the knees fully extended [24]. When performing the Beighton assessment, a Baseline HiRes 360° goniometer was used to accurately evaluate the ranges of motion. A positive joint movement is scored as 1 point, while a negative result is scored as 0 points. In the present study, a Beighton score cutoff value of ≥ 5/9 was applied [24].
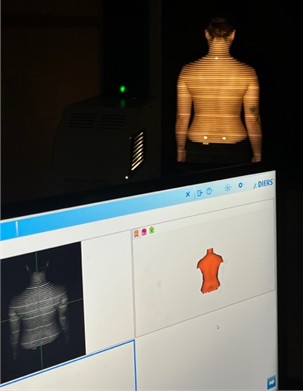
Participants' posture was assessed using the Diers Formetric 4D system. Three reflective markers were placed on the participant’s exposed back to serve as anatomical landmarks, enabling accurate determination of the spatial position of spinal segments. One marker was placed over the spinous process of the C7 vertebra, while the other two were positioned over the posterior superior iliac spines (PSIS). During the assessment, participants stood at a distance of 2 m from the scanner, which projected horizontal light lines onto the surface of the back. These lines were distributed according to the contours of the underlying bony structures (vertebrae, pelvis, and other anatomical landmarks) as well as the positions of the reflective markers. The captured image was processed using specialized software and reconstructed as a three-dimensional (3D) topographic model of the spine in the sagittal, frontal, and transverse planes. Participants were instructed to expose their back, relax, look straight ahead at a point on the wall, breathe normally, and stand upright barefoot with their feet positioned hip-width apart on a marked line (Fig. 1). The following posture parameters were selected for analysis [25]: sagittal imbalance, thoracic kyphosis angle, lumbar lordosis angle, pelvic torsion, pelvic rotation, vertebral rotation.
Fig. 1Posture assessment using the Diers Formetric 4D system
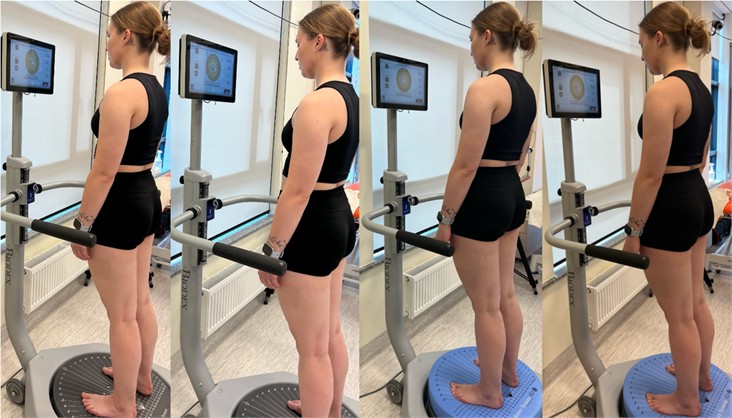
Balance performance was measured with the Biodex Balance System SD, version 4.x. Static balance was tested using the Modified Clinical Test of Sensory Integration and Balance, which includes four testing conditions: eyes open and eyes closed on a firm surface, and eyes open and eyes closed on an unstable surface. For the unstable-surface conditions, a dedicated circular platform designed for the Biodex Balance System SD was placed on the system base (Fig. 2).
Each task lasts 30 seconds, with a 10-second break between tasks. The overall normative mean sway index for all four test conditions is 1.11. The further the participants’ overall result for these four test conditions deviates from this normative value, the more impaired balance may be suspected; that is, a higher overall sway index value across all four test conditions indicates greater balance instability among the participants [26, 27]. The overall result of all four test tasks was used for data analysis.
Fig. 2Static balance testing under four conditions with the Modified Clinical Test of Sensory Integration and Balance on the Biodex Balance System, version 4.x
2.3. Data analysis
Statistical processing was carried out with IBM SPSS Statistics 31.0. The distribution of the data was checked using the Shapiro-Wilk test. For comparisons of two independent groups, Student’s t-test was applied when the assumption of normality was satisfied, whereas the Mann-Whitney-Wilcoxon test was selected for non-normally distributed data. Variables meeting parametric assumptions are reported as mean () and standard deviation (SD), expressed as m (SD). Non-parametric variables are summarized as median (Md), interquartile range (IQR), and mean (m), expressed as Md (Q1-Q3; m). The threshold for statistical significance was defined as 0.05.
3. Results
The characteristics of body posture were analysed based on six parameters, which included the assessment of spinal and pelvic positions in different planes, in order to compare body posture between the study and control groups.
After evaluating the results of sagittal imbalance, the median value in the study group was 1 degree, while the median value in the control group was 2 degrees. When comparing the results of sagittal imbalance between the groups, no statistically significant difference was found (see Table 1).
When analysing the data on the thoracic kyphosis angle, the mean value of the results obtained in women assigned to the study group was 49.44 degrees, while in women assigned to the control group it was 48.68 degrees. The thoracic kyphosis angle did not differ statistically significantly between the study and control groups.
When assessing the lumbar lordosis angle, the mean value in the study group was 47.31 degrees, while the mean value in the control group was 48.59 degrees. When comparing the two groups, the obtained results did not differ significantly.
Analysis of pelvic torsion in the sagittal plane showed that the median value was 2 degrees in both the GJH and control groups. Despite identical median values, comparison between the groups revealed a statistically significant difference, indicating higher sagittal-plane pelvic torsion values among women with GJH.
Table 1Comparison of postural parameters between the study and control groups
Postural parameters | Study group | Control group | Comparison between groups |
Numerical characteristics | |||
Sagittal imbalance | 1 (1-2; 1.9) | 2 (1-3; 1.81) | 760.5; 0.677 |
Thoracic kyphosis angle | 49.44 (10.50) | 48.68 (9.76) | 0.326; 0.745 |
Lumbar lordosis angle | 47.31 (10.46) | 48.59 (11.15) | –0.519; 0.605 |
Pelvic torsion angle in the sagittal plane | 2 (1-4; 2.82) | 2 (0.5-3; 1.78) | 532.0; 0.044 |
Pelvic rotation in the horizontal plane | 2 (1-4; 2.49) | 2 (2-4; 2.70) | 777.0; 0.556 |
Spinal rotation | 3 (2-3; 3.03) | 2 (2-3; 2.46) | 678.0; 0.639 |
When assessing the results of pelvic rotation in the horizontal plane, the median value in the study group was 2 degrees, while in the control group it was 2 degrees. When comparing these groups, the results showed that pelvic rotation did not differ statistically significantly between the two groups.
When analysing the spinal rotation data, the median value in the study group was 3 degrees, while in the control group it was 2 degrees. When comparing the study and control groups, no statistically significant difference was found.
The overall static balance score across the four testing conditions – eyes open on a stable surface, eyes closed on a stable surface, eyes open on an unstable surface, and eyes closed on an unstable surface – was higher in the GJH group, with a median value of 2.34 (2.20-2.72; 2.53) points, compared with 1.80 (1.56-1.89; 1.74) points in the control group (Fig. 3).
Fig. 3Comparison of the outcomes of the modified Clinical Test of Sensory Integration and Balance *–p< 0.05
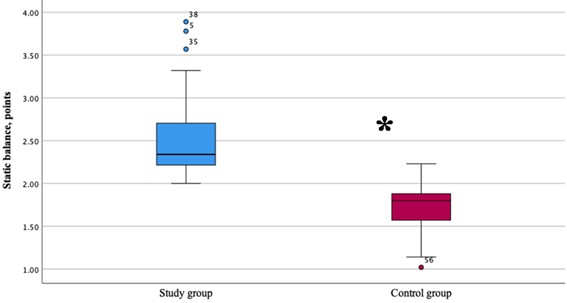
A statistically significant between-group difference was identified for static balance ( 28.5; 0.001), indicating poorer static balance among women with GJH.
4. Discussion
A study conducted by Yildiz and co-authors showed that the posture of individuals with GJH was poorer than that of individuals without GJH [16]. The results obtained in the study by Hershkovich et al. showed that spinal deformities may be identified more frequently in individuals with GJH than in those without this characteristic [17]. However, scientific publications present varying research findings, in some studies, no significant differences were found between individuals with and without GJH. For example, in the scientific study conducted by Czaprowski and co-authors, it was observed that body posture in individuals with GJH did not differ from that of individuals without GJH [28].
In our study, of the six body posture indicators assessed, only one statistically significant difference was found: the pelvic torsion angle in the sagittal plane was greater in women with GJH than in women without GJH. When evaluating all body posture indicators analyzed in this study, it can be stated that women with GJH had a greater pelvic torsion angle in the sagittal plane, whereas no significant differences between the groups were found in the analysis of the other five indicators.
Researchers investigating balance in individuals with GJH state in their studies that both static and dynamic balance may be impaired due to increased joint ranges of motion. This statement is supported by a study, which found that GJH may be associated with poorer static and dynamic balance control [29]. In another study conducted by Juul-Kristensen and co-authors, it was found that individuals with GJH demonstrated greater body sway during the assessment of static balance than participants without GJH [21]. Meanwhile, in the study conducted by Zong-Chen and co-authors, it was observed that dynamic balance control was poorer in individuals with GJH than in those without this characteristic [30].
After analyzing the results obtained in our study, it was found that static balance was poorer in women with GJH compared with those without GJH. The results of our study also support the hypothesis that individuals with GJH may have poorer balance than individuals without GJH.
Taking into account the obtained study results, it can be emphasised that it is appropriate to comprehensively assess body posture and balance in individuals with GJH. One of the main strengths of this study is the use of modern and objective assessment equipment. The application of these tools in the assessment of body posture and balance in women with GJH is rarely found in research, therefore, this study is novel and may be useful for further scientific work. We observed that, in order to provide a more comprehensive explanation of the obtained study results, it would be useful to have additional information on the participants’ musculoskeletal characteristics. One limitation of the study was that participants’ pain experience was not assessed. To comprehensively evaluate body posture in individuals with and without GJH, the assessment should also include the cervical spine, lower limbs, and other postural parameters, however, the capabilities of the system used in our study to perform such assessments were limited.
5. Conclusions
The indicators of sagittal imbalance, thoracic kyphosis angle, lumbar lordosis angle, pelvic rotation, and vertebral rotation were similar between women with and without generalized joint hypermobility, however, the pelvic torsion angle in the sagittal plane was greater in the group of women with generalized joint hypermobility. Static balance was poorer in the group of women with generalized joint hypermobility.
References
-
B. T. Tinkle, “Symptomatic joint hypermobility,” Best Practice and Research Clinical Rheumatology, Vol. 34, No. 3, p. 101508, 2020, https://doi.org/10.1016/j.berh.2020.101508
-
M. Castori, B. Tinkle, H. Levy, R. Grahame, F. Malfait, and A. Hakim, “A framework for the classification of joint hypermobility and related conditions,” American Journal of Medical Genetics Part C: Seminars in Medical Genetics, Vol. 175, No. 1, pp. 148–157, Feb. 2017, https://doi.org/10.1002/ajmg.c.31539
-
M. M. Lamari et al., “Generalized joint hypermobility: a statistical analysis identifies non-axial involvement in most cases,” Children, Vol. 11, No. 3, p. 344, Mar. 2024, https://doi.org/10.3390/children11030344
-
C. Gensemer, R. Burks, S. Kautz, D. P. Judge, M. Lavallee, and R. A. Norris, “Hypermobile Ehlers-Danlos syndromes: complex phenotypes, challenging diagnoses, and poorly understood causes,” Developmental Dynamics, Vol. 250, No. 3, pp. 318–344, 2020, https://doi.org/10.1002/dvdy.220
-
M. Glans, N. Thelin, M. B. Humble, M. Elwin, and S. Bejerot, “Association between adult attention-deficit hyperactivity disorder and generalised joint hypermobility: a cross-sectional case control comparison,” Journal of Psychiatric Research, Vol. 143, pp. 334–340, Nov. 2021, https://doi.org/10.1016/j.jpsychires.2021.07.006
-
L. Blajwajs, J. Williams, W. Timmons, and J. Sproule, “Hypermobility prevalence, measurements, and outcomes in childhood, adolescence, and emerging adulthood: a systematic review,” Rheumatology International, Vol. 43, No. 8, pp. 1423–1444, May 2023, https://doi.org/10.1007/s00296-023-05338-x
-
C. Baeza-Velasco, L. Sinibaldi, and M. Castori, “Attention-deficit/hyperactivity disorder, joint hypermobility-related disorders and pain: expanding body-mind connections to the developmental age,” ADHD Attention Deficit and Hyperactivity Disorders, Vol. 10, No. 3, pp. 163–175, 2018, https://doi.org/10.1007/s12402-018-0252-2
-
A. Schlager, K. Ahlqvist, R. Pingel, L. Nilsson-Wikmar, C. B. Olsson, and P. Kristiansson, “Validity of the self-reported five-part questionnaire as an assessment of generalized joint hypermobility in early pregnancy,” BMC Musculoskeletal Disorders, Vol. 21, No. 1, p. 514, Aug. 2020, https://doi.org/10.1186/s12891-020-03524-7
-
L. N. Bockhorn, A. M. Vera, D. Dong, D. A. Delgado, K. E. Varner, and J. D. Harris, “Interrater and intrarater reliability of the Beighton score: a systematic review,” Orthopaedic Journal of Sports Medicine, Vol. 9, No. 1, p. 2325967120968099, Jan. 2021, https://doi.org/10.1177/2325967120968099
-
A. Hakim and R. Grahame, “A simple questionnaire to detect hypermobility: an adjunct to the assessment of patients with diffuse musculoskeletal pain,” International Journal of Clinical Practice, Vol. 57, No. 3, pp. 163–166, Apr. 2003, https://doi.org/10.1111/j.1742-1241.2003.tb10455.x
-
D. Syx, I. de Wandele, L. Rombaut, and F. Malfait, “Hypermobility, the Ehlers-Danlos syndromes and chronic pain,” Clinical and Experimental Rheumatology, Vol. 35, No. 5, pp. 116–122, 2017.
-
S. Malek, E. J. Reinhold, and G. S. Pearce, “The Beighton score as a measure of generalised joint hypermobility,” Rheumatology International, Vol. 41, No. 10, pp. 1707–1716, Mar. 2021, https://doi.org/10.1007/s00296-021-04832-4
-
L. L. Nicholson et al., “International perspectives on joint hypermobility: a synthesis of current science to guide clinical and research directions,” Journal of Clinical Rheumatology, Vol. 28, No. 6, pp. 314–320, 2022.
-
B. Juul‐Kristensen, K. Schmedling, L. Rombaut, H. Lund, and R. H. H. Engelbert, “Measurement properties of clinical assessment methods for classifying generalized joint hypermobility-A systematic review,” American Journal of Medical Genetics Part C: Seminars in Medical Genetics, Vol. 175, No. 1, pp. 116–147, 2017, https://doi.org/10.1002/ajmg.c.31540
-
M. B. Carroll, “Hypermobility spectrum disorders: a review,” Rheumatology and Immunology Research, Vol. 4, No. 2, pp. 60–68, Jul. 2023, https://doi.org/10.2478/rir-2023-0010
-
R. Yıldız and A. Yıldız, “Evaluation of postural habits and awareness in young adults with generalized joint hypermobility,” (in Turkish), Ergoterapi Ve Rehabilitasyon Dergisi, Vol. 13, No. 3, pp. 186–192, 2025, https://doi.org/10.30720/ered.1543835
-
O. Hershkovich, B. Gordon, E. Derazne, D. Tzur, A. Afek, and R. Lotan, “Hypermobility among adolescents and the association with spinal deformities: a large cross-sectional study,” JAAOS: Global Research and Reviews, Vol. 8, No. 7, p. e24, 2024, https://doi.org/10.5435/jaaosglobal-d-24-00047
-
L. Vargas, H. H. Huang, Y. Zhu, and X. Hu, “Static and dynamic proprioceptive recognition through vibrotactile stimulation,” Journal of Neural Engineering, Vol. 18, No. 4, p. 046093, Aug. 2021, https://doi.org/10.1088/1741-2552/ac0d43
-
M. Scheper et al., “The association between muscle strength and activity limitations in patients with the hypermobility type of Ehlers-Danlos syndrome: the impact of proprioception,” Disability and Rehabilitation, Vol. 39, No. 14, pp. 1391–1397, Jul. 2017, https://doi.org/10.1080/09638288.2016.1196396
-
E. Aydın, “Postural balance control in women with generalized joint laxity,” Turkish Journal of Physical Medicine and Rehabilitation, Vol. 63, No. 3, pp. 259–265, Sep. 2017, https://doi.org/10.5606/tftrd.2017.160
-
B. Juul-Kristensen, K. Johansen, P. Hendriksen, P. Melcher, J. Sandfeld, and B. Jensen, “Girls with generalized joint hypermobility display changed muscle activity and postural sway during static balance tasks,” Scandinavian Journal of Rheumatology, Vol. 45, No. 1, pp. 57–65, Jan. 2016, https://doi.org/10.3109/03009742.2015.1041154
-
O. A. Ituen, J. Duysens, G. Ferguson, and B. Smits-Engelsman, “The strength of balance: strength and dynamic balance in children with and without hypermobility,” PLOS ONE, Vol. 19, No. 6, p. e0302218, Jun. 2024, https://doi.org/10.1371/journal.pone.0302218
-
M. Liu et al., “Study on the balance and gait characteristics of subjects with generalized joint hypermobility residing in high-altitude using wearable devices: a cross-sectional study,” BMC Musculoskeletal Disorders, Vol. 25, No. 1, p. 837, Oct. 2024, https://doi.org/10.1186/s12891-024-07883-3
-
F. Malfait et al., “The 2017 international classification of the Ehlers-Danlos syndromes,” American Journal of Medical Genetics Part C: Seminars in Medical Genetics, Vol. 175, No. 1, pp. 8–26, Mar. 2017, https://doi.org/10.1002/ajmg.c.31552
-
B. F. Degenhardt, Z. Starks, and S. Bhatia, “Reliability of the DIERS Formetric 4D spine shape parameters in adults without postural deformities,” BioMed Research International, Vol. 2020, No. 1, p. 1796247, Feb. 2020, https://doi.org/10.1155/2020/1796247
-
N. Dawson, D. Dzurino, M. Karleskint, and J. Tucker, “Examining the reliability, correlation, and validity of commonly used assessment tools to measure balance,” Health Science Reports, Vol. 1, No. 12, p. e98, Oct. 2018, https://doi.org/10.1002/hsr2.98
-
Balance System SD (with v4.X software): Operation/Service Manual. New York, NY, USA: Biodex Medical Systems, Inc., 2017.
-
D. Czaprowski and P. Pawłowska, “The influence of generalized joint hypermobility on the sagittal profile of the spine in children aged 10-13 years,” Ortopedia Traumatologia Rehabilitacja, Vol. 15, No. 6, pp. 545–553, 2013, https://doi.org/10.5604/15093492.1091510
-
R. Kocheta, R. Musale, and N. Andhare, “Correlation between joint hypermobility and balance in Indian elite gymnasts,” Archives of Medicine and Health Sciences, Vol. 11, No. 2, pp. 219–222, Oct. 2023, https://doi.org/10.4103/amhs.amhs_64_23
-
Z.-C. Hou et al., “Balance training benefits chronic ankle instability with generalized joint hypermobility: A prospective cohort study,” BMC Musculoskeletal Disorders, Vol. 24, No. 1, p. 71, Jan. 2023, https://doi.org/10.1186/s12891-023-06179-2
About this article

The authors have not disclosed any funding.
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Kamilė Pilvinytė: data curation, investigation, project administration, visualization, writing-original draft. Algė Daunoravičienė: conceptualization, methodology, supervision, writing-review and editing. Ernesta Gurskienė: investigation, methodology, validation. Ernesta Aukštuolytė-Bačienė: formal analysis, investigation, resources, supervision, writing-review and editing.
The authors declare that they have no conflict of interest.
The research adhered to all applicable laws and ethics standards. Permission to perform clinical trials investigation was granted by Bioethics Center of the Lithuanian University of Health Sciences, No. 2026-BEC2-0204, 2026 02 13. Participants provided written informed consent prior to the research.
