Abstract
Whole body vibration is a novel modality that has been proposed as a potentially useful adjunct to exercise to improve various aspects of musculoskeletal function. The purpose of this study was to determine the effect of adding whole body vibration to a conventional exercise program to improve balance in elderly independently living women. A total of 40 elderly women, randomly divided into two equal groups (exercise and vibration versus exercise only) participated in an 8-week physiotherapy program for falls prevention. Participants in both groups performed the same exercise program twice per week. The participants in the vibration group also performed exercises on a vertical vibration platform set at a 27 Hz frequency and 3 mm amplitude. Standard tests to assess balance were performed before and after the intervention to monitor changes. Performance on all balance tests was significantly improved for both groups after the intervention (P < 0.05), however there were no significant differences in improvement between groups.
1. Introduction
All European countries are experiencing significant ageing of the population. Falls in older adults are a major public health concern [1] and a primary cause of morbidity and disability [2]. More than one-third of persons 65 years of age or older fall each year, and in half of these individuals, falls become recurrent [2]. Various interventions, such as balance training exercises, home modifications, appropriate footwear, and walking aids, have been proposed to promote health, enhance quality of life, and reduce falls in older people.
Whole-body vibration (WBV) is a novel adjunct to exercise that is currently being tested in sports, geriatrics, and rehabilitation [3]. It has recently become especially popular in European health and fitness clubs as an alternative training method [4]. WBV training consists of performing static and dynamic exercises on a vibrating platform and as such may have potential to be used to complement standard physical rehabilitation programs to improve function, especially balance [5, 6]. The results of previous intervention studies suggest that controlled WBV can improve elements of fall risk in elderly patients [7] and can be beneficial to improve balance and mobility in nursing home residents [8], but other studies have not shown benefits from using WBV [9, 10]. Therefore, the benefits of WBV training on balance in independently living elderly women are still unclear.
The aim of this study was to assess the effect of adding WBV exercises to a standard fall prevention program intervention to improve balance in elderly independently living women.
2. Methods
2.1. Participants
Subjects were recruited from the Social Service Centre of Kaunas District. Forty women (mean ± SD age: 67.7 ± 4.1 years) met the inclusion criteria and agreed to participate in the study. The inclusion criteria were: age between 60 and 74 years, living independently, no known neurological disorders, and no contraindications to vibration exposure (pacemaker, current kidney or gall stones, acute lower back pain, blood clot or thrombosis within the last six months, fracture or joint replacement within the past 12 months, vibration-related injuries, amputation of lower extremities other than toes, diabetes mellitus, tumors).
The subjects, matched for age, were randomly divided into two groups: exercise and vibration ( 20) and exercise ( 20).
2.2. Intervention
Subjects from both groups participated in an 8-week (50 minute exercise sessions twice a week) physiotherapy program for falls prevention. The physiotherapy program consisted of strengthening, flexibility, postural control, balance and endurance exercises. In addition to the standard exercise program, the individuals in the group receiving WBV performed an additional six exercises while standing on a vertical vibration platform (VibraFit Medic, made in Germany) set at a 27 Hz frequency and 3 mm amplitude (Figure 1).
Fig. 1Vibration platform VibraFit Medic

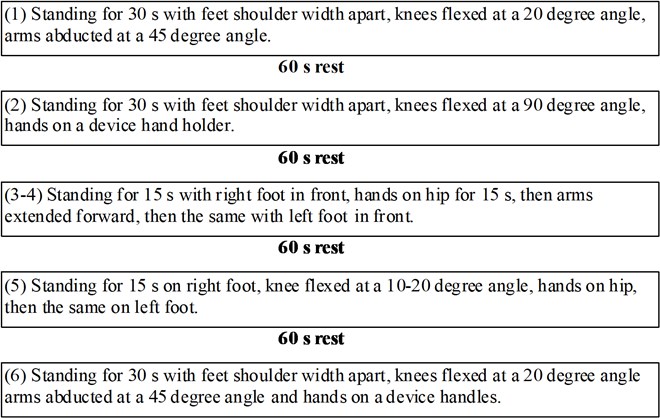
The 6 static exercises performed on the platform targeted the lower limb muscles (Figure 2).
Fig. 2Vibration protocol
2.3. Outcome measures
30-s chair stand test [11]. This test assesses leg strength and endurance and is designed to test the functional fitness of seniors. The subject sits in the middle of the seat (chair without arm rests, 44 cm high) with feet shoulder width apart, feet flat on the floor. The arms are crossed and held close to the chest. From the sitting position, the subject stands up and then sits back down (up and down equals one stand). This is repeated for 30 seconds. The total number of complete chair stands performed within 30 seconds is counted. If the subject has completed a full stand from the sitting position when the time elapses, the final stand is counted in the total.
Modified clinical test for sensory interaction of balance [12]. This tool assesses a person’s ability to use somatosensory, visual, and vestibular inputs for balance. The test has also been used to determine fall risk in older adults. Subjects were asked to stand with their arms folded across their chest and their feet together for 30 seconds in each of 4 test conditions: (1) stand on a firm surface with eyes open, (2) stand on a firm surface with eyes closed, (3) stand on a compliant foam surface with eyes open, and (4) stand on a compliant foam surface with eyes closed. The 4 conditions were performed with shoes off. The amount and direction of the subject‘s body sway over the 4 conditions were observed. Every condition was scored as 0 (large sway and difficulties in keeping balance) or 1 (stable, very small sway). Balance evaluation in all 4 conditions was summed.
Timed up and go test [13]. The original purpose of the test was to test basic functional mobility skills and fall risk in the elderly. The test requires a subject to stand up from a chair, walk 3 m, turn, walk back, and sit down. The time taken to complete the test is recorded.
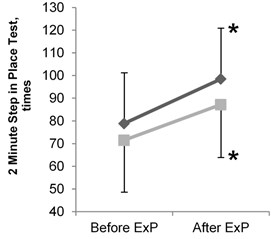
2 minute step in place test [14]. This test is designed to assess the level of functional fitness of seniors by measuring aerobic endurance. The subject stands up next to the wall where the level corresponding to the height midway between the patella and iliac crest has been marked with a piece of tape. The subject then marches in place for two minutes, lifting the knees to the height of the tape. Resting is allowed, and holding onto the wall or a stable chair is allowed. The total number of times the right knee reaches the tape level in two minutes is recorded.
Dynamic gait index [15]. This test was developed as a clinical tool to assess gait, balance, and fall risk. It evaluates not only usual steady-state walking, but also walking during more challenging tasks. Eight functional walking tasks (gait level surface, change in gait speed, gait with horizontal and vertical head turns, gait and pivot turn, step-over and around obstacle, walk upstairs) are performed by the subject. A four-point ordinal scale, ranging from 0-3, is used for scoring: 0 indicates the lowest level of function and 3 the highest level of function. The highest individual score possible is 24. Scores of 19 or less have been related to increase incidence of falls.
All tests were performed at baseline and after the 8-week intervention.
2.4. Statistical analysis
Quantitative variables were expressed as mean ± standard deviation (SD). Differences in baseline characteristics between the two groups was assessed using Mann-Whitney test, and changes between before and after intervention − Wilcoxon test. All subjects completed the study, so no adjustments were needed for drop-outs.
All analyses were performed using SPSS version 19. The difference across groups and trials were considered statistically significant when values were less than 0.05.
3. Results
The results of balance tests in elderly women before and after the intervention are presented in Table 1.
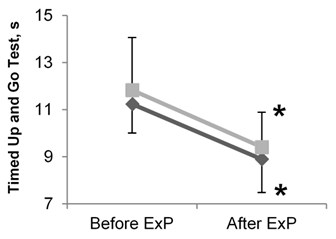
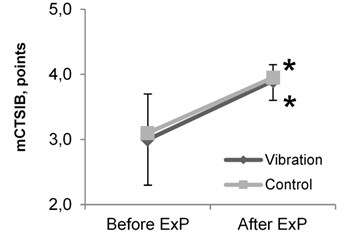
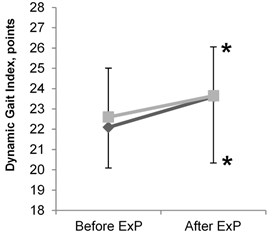
After the 8 week intervention, both groups demonstrated a significant increase in the number of completed chair stands in 30 seconds ( 0.05), the score on the Modified Clinical Test for Sensory Interaction of Balance ( 0.05), the total number of times the right knee reached the tape level in the 2 Minute Step in Place Test ( 0.05), and the score on the Dynamic Gait Index used to assess the ability to walk and change directions ( 0.05) (Table 1, Figures 3b, 3c, 3d). After the intervention, both groups also showed a significant reduction in the amount of time needed to complete the Timed Up and Go Test ( 0.05) (Table 1, Figure 3a).
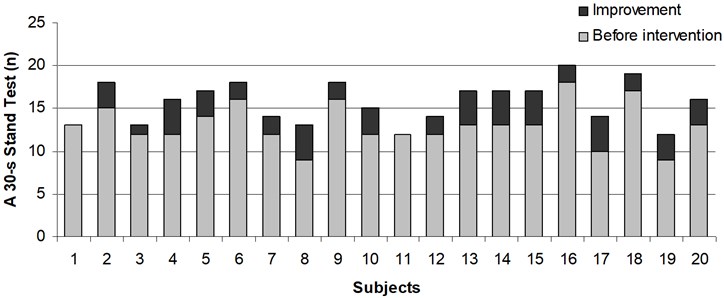
There were no significant differences between groups before and after the intervention in all completed balance tests, with both groups displaying a similar improvement post-intervention (Figure 4 and Figure 5).
Table 1Results of balance tests in elderly women before and after the intervention
Measurements | Before intervention | After 8 week intervention | ||
Control Group (PT program) | Vibration group (PT program + WBV exercise) | Control group (PT program) | Vibration group (PT program + WBV exercise) | |
A 30-s chair stand test (n) | 13.9±2.4 | 14.5±2.0 | 16.8±2.4* | 17.4±3.3* |
mCTSIB (0-4) | 3.1±0.6 | 3.0±0.7 | 4.0±0.2* | 3.9±0.3* |
Timed up and go test (s) | 11.8±2.2 | 11.2±1.2 | 9.4±1.5* | 8.9±1.4* |
2 minute step in place test (n) | 71.5±22.9 | 78.9±22.3 | 87.2±23.3* | 98.5±22.4* |
Dynamic gait index (0-24) | 22.6±2.4 | 22.1±2.0 | 23.7±2.4* | 23.6±3.3* |
PT – physiotherapy; WBV – whole body vibration; mCTSIB – Modified Clinical Test for Sensory Interaction of Balance; * – difference within group is significant ( 0.05) | ||||
Fig. 3Results of balance tests in elderly women before and after the intervention: a) results of timed up and go test; b) results of modified clinical test for sensory interaction of balance (mCTSIB); c) results of dynamic gait index; d) results of 2 minute step in place test. ExP – exercise program; * – difference within groups is significant (P< 0.05)
a)
b)
c)
d)
Fig. 4Improvement in a 30-s chair stand test in every subject of vibration group
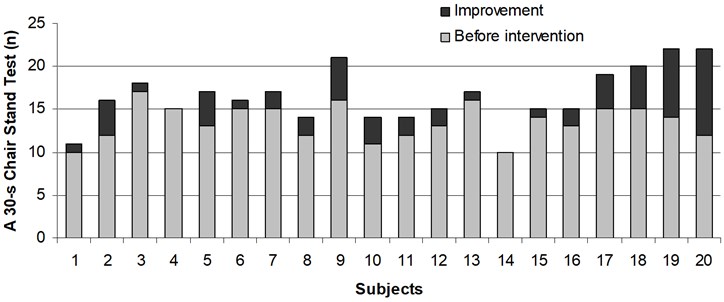
Fig. 5Improvement in a 30-s chair stand test in every subject of control group
4. Discussion
The present study investigated the potential added benefits of using WBV as a supplement to an 8-week fall prevention program to improve balance in independently living elderly women. The absence of individuals dropping-out of the study suggest that the WBV exercises were safely administered and were well tolerated as part of a short-term intervention program in an elderly population [16]. At the conclusion of the 8-week intervention, significant improvement ( 0.05) was noted for both groups on all outcome measures. However, there was no difference between groups at either pre or post-intervention, indicating that the addition of WBV exercises to the fall prevention program did not result in any additional benefits based on our outcome measures. These results contrast with the findings of previous publications [17, 18].
Kawanabe et al. [17] previously reported that 8 weeks of a combination of WBV and routine exercises significantly improved walking speed and balance in the elderly, while no significant changes in these parameters were observed in those only performing the routine exercises. Similarly, Simao et al. [18] showed the benefits of 12 weeks of WBV exercises on physical function in the elderly, as measured with the 6-minute walk test, the Berg Balance Scale, and gait speed. In contrast, our findings are in agreement with the conclusion by Iwamoto et al. [19] who demonstrated the beneficial effect of an exercise program aimed at improving flexibility, body balance, muscle power, and walking ability in preventing falls in the elderly. Our results are also consistent with the conclusion of a recent literature review suggesting that WBV exercises have little or no effect on muscular function, balance, and bone mass, and are not superior to other interventions [20].
Two types of sinusoidal WBV devices, vertical vibration and side-to-side vibration, are available for training that aim to improve balance in the elderly. Based on a previous systematic review, training using vertical vibration seems to have only small effects on static and dynamic balance, while side to side vibration has shown to result in small to moderate improvements in balance [21]. Bautman et al. [8], who have applied vertical vibration, as we did in our study, found that 6 weeks static WBV exercises are feasible in elderly nursing home residents with limited functional dependency, and might be beneficial for balance and mobility. Similarly, Cheung et al. [9] found that 3 months of WBV was effective in improving the balancing ability in elderly women. Finally, Sitja-Rabert et al. [6] in a different systematic review concluded that WBV training may improve strength, power, and balance in comparison with a control group, although these effects are not apparent when compared with a group that does conventional exercise.
Several studies have shown the beneficial effects of WBV exercise on the musculoskeletal system. It has been shown to improve balance, endurance capacity, walking at preferred speed (10 m walk test), Timed up and Go, lower limb muscle function, and hip bone density in postmenopausal women [9, 22, 23, 24]. However, the duration of the intervention in these studies was much longer (from 3 to 8 months) than in our study and in most studies either lower (from 12.5 to 20 Hz) or higher (from 35 to 40 Hz) vibration frequencies were used. In contrast, Bogaerts et al. [10] did not find an additional benefit of WBV training on fall risk and postural control, despite the improvements in endurance capacity and walking at preferred speed in the elderly women they studied.
We acknowledge certain limitations of our study. The relatively small number of participants, limiting the power of the study, may have decreased our ability to determine differences between groups. The short duration of the intervention may have limited the ability to see differences over time. Finally the lack of a vibration-only group limits the ability to interpret the effectiveness of WBV exercises provided in isolation.
5. Conclusion
The results of the present study showed that the addition of WBV exercises to an 8-week fall prevention exercise program did not result in additional gain in balance and mobility for elderly independently living women. Both groups in the study showed significant but similar improvement in balance after the 8-week intervention. Future investigations are required to explore the potential of vibration for improving balance and preventing falls in elderly women.
6. Competing interests
The authors declare that they have no competing interests.
References
-
Gillespie L. D., Robertson M. C., Gillespie W. J. et al. Interventions for preventing falls in older people living in the community. Cochrane Database of Systematic Reviews 2009, CD007146.
-
Tinetti M. E., Kumar C. The patient who falls: “It’s always a trade-off”. JAMA, Vol. 303, Issue 3, 2010, p. 258-266.
-
Russo C. R., Lauretani F., Bandinelli S. et al. High-frequency training increases muscle power in postmenopausal women. Arch. Phys. Med. Rehabil., Vol. 84, 2003, p. 1854-1857.
-
Delecluse Ch., Roelants M., Verschueren S. Strength increase after whole-body vibration compared with resistance training. Med. Sci. Sports Exerc., Vol. 35, Issue 6, 2003, p. 1033-1041.
-
Sitjà-Rabert M., Martínez-ZapataJ., Fort-Vanmeerhaeghe A. et al. Whole body vibration for older persons: an open randomized, multicentre, parallel, clinical Arial. BMC Geriatrics, Vol. 11, 2011, p. 89, http://www.biomedcentral.com/1471-2318/11/89.
-
Sitjà-Rabert M., Rigau D., Fort Vanmeerghaeghe A. et al. Efficacy of whole body vibration exercise in older people: a systematic review. Disabil. Rehabil., Vol. 34, Issue 11, 2012, p. 883-893.
-
Bruyère O., Wuidart M. A., Di Palma E. et al. Controlled whole body vibration to decrease fall risk and improve health-related quality of life of nursing home residents. Arch. Phys. Med. Rehabil., Vol. 86, 2005, p. 303-307.
-
Bautmans I., Van Hees E., Lemper J., Mets T. The feasibility of whole body vibration in institutionalised elderly persons and its influence on muscle performance, balance and mobility: a randomised controlled trial. BMC Geriatr., Vol. 5, 2005, p. 17.
-
Cheung W. H., Mok H. W., Qin L. et al. High-frequency whole-body vibration improves balancing ability in elderly women. Arch. Phys. Med. Rehabil., Vol. 88, Issue 7, 2007, p. 852-857.
-
Bogaerts A., Delecluse C., Boonen S. et al. Changes in balance, functional performance and fall risk following whole body vibration training and vitamin D supplementation in institutionalized elderly women. A 6 month randomized controlled trial. Gait Posture, Vol. 33, Issue 3, 2011, p. 466-472.
-
Jones C. J., Rikli R. E., Beam W. C. A 30-s chair-stand test to measure lower body strength in community-residing older adults. J. of Aging & Physical Activity, Vol. 8, 2000, p. 85.
-
Shumway-Cook A., Horak F. B. Assessing the influence of sensory integration on balance. Suggestions from the field. Phys. Ther., Vol. 66, 1986, p. 1548-1549.
-
Podsiadlo D., Richardson S. The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc., Vol. 39, 1991, p. 142-148.
-
Jones C. J., Rikli R. E. Measuring functional fitness of older adults. The Journal on Active Aging, Vol. 2, 2002, p. 24-30.
-
Wrisley D. M., Marchett G. F., Kuharsky D. K. et al. Reliability, internal consistency, and validity of data obtained with the functional gait assessment. Phys. Ther., Vol. 84, 2004, p. 906-918.
-
Carlucci F., Mazzà C., Cappozzo A. Does whole-body vibration training have acute residual effects on postural control ability of elderly women? J. Strength Cond. Res., Vol. 24, Issue 12, 2010, p. 3363-3368.
-
Kawanabe K., Kawashima A., Sashimoto I. et al. Effect of whole-body vibration exercise and muscle strengthening, balance, and walking exercises on walking ability in the elderly. Keio J. Med., Vol. 56, Issue 1, 2007, p. 28-33.
-
Simão A. P., Avelar N. C., Tossige-Gomes R. et al. Functional performance and inflammatory cytokines after squat exercises and whole-body vibration in elderly individuals with knee osteoarthritis. Arch. Phys. Med. Rehabil., 2012.
-
Iwamoto J., Suzuki H., Tanaka K. et al. Preventative effect of exercise against falls in the elderly: a randomized controlled trial. Osteoporos Int., Vol. 20, Issue 7, 2009, p. 1233-1240.
-
Lohse G., Nilsagård Y. Effects of whole body vibration – a systematic review of randomized, controlled trials. 2009, http://www.orebroll.se.
-
Rogan S., Hilfiker R., Herren K. et al. Effects of whole-body vibration on postural control in elderly: a systematic review and meta-analysis. BMC Geriatr., Vol. 11, 2011, p. 72.
-
Verschueren S. M., Roelants M., Delecluse C. et al. Effect of 6-month whole body vibration training on hip density, muscle strength, and postural control in postmenopausal women: a randomized controlled pilot study. J. Bone Miner. Res., Vol. 19, Issue 3, 2004, p. 352-359.
-
Gusi N., Raimundo A., Leal A. Low-frequency vibratory exercise reduces the risk of bone fracture more than walking: a randomized controlled trial. BMC Musculoskelet. Disord., Vol. 7, 2006, p. 92.
-
Beck B. R., Norling T. L. The effect of 8 months of twice-weekly low- or higher intensity whole body vibration on risk factors for postmenopausal hip fracture. Am. J. Phys. Med. Rehabil., Vol. 89, Issue 12, 2010, p. 997-1009.
About this article

