Abstract
The paper presents a microprocessor force recorder, whose design allows the measurement of occlusal forces on a continuous basis with a maximum frequency of 250 Hz. The electronic dental dynamometer records the results of clinical trials in the form of graphic images and text files which are presented directly onto the computer. The recorded results can be processed digitally, as well as compared with other measurements, resulting in the ability to monitor the progress and potential advances in the treatment of masticatory organ diseases. An important advantage of the proposed solution is the simple and intuitive design. In addition, the dynamometer requires no power coming directly from the electricity network, as it is powered through a 5 V USB port. This feature not only determines the comfort of use, but also the safety as the voltage does not pose a risk to the patient during examination. The results recorded during clinical trials using the electronic dental dynamometer are consistent with those obtained using a calibrated mechanical dental dynamometer.
1. Introduction
An important element in determining a reliable assessment of passive and active forces connected with the exercise capacity of masticatory muscles is to determine the actual value of occlusal forces. Knowledge of the size and distribution of occlusal forces provides the dentist with relevant information, as occlusal disorders are one of the causes of dysfunction, which in turn leads to malfunction of the temporomandibular joints. In order to formulate a credible and reliable diagnosis, the dentist should have a specialized device that should be characterized by the simplicity and functionality of use. The main factors affecting the value of recorded occlusal forces include the hardness of tooth contact with the sensing element and the degree of opening of dental arches [1].
It has been found [2] that the hardness of the material from which the dynamometer overlays are made has a significant impact on the value of the measured force. In clinical trials, the most commonly used are silicone or plastic overlays. Conducted observations indicate that the contact surface of the occlusal or incisor edges with hard plastic causes a reduction in the occlusal forces recorded. This limitation is related to the functioning of the mechanoreceptors located within the teeth. It should be noted that during the study of occlusal forces, the design of the dynamometer can significantly affect the measurement results. For example, mechanical dynamometers [3], as well as design solutions based on strain gauges [4] and dynamometers [5], require a wider opening of the dental arches, the scope of which is in the range from 11 to 15 mm [6-8]. Such an orientation of the dental arches has a decisive influence on the configuration of the heads of the condylar process and articular discs within the temporomandibular joints [9-12]. For this reason, dental dynamometers should be designed in such a way that the degree of dental arch opening should be as small as possible. The method of measurement of occlusal forces, with minimal opening of the dental arches, which uses a sensitive pressure method, has been proposed [13]. Such registered measurements are the basis for image analysis on the Occluzer FDP-707 scanner. Despite the undoubted advantages, such as the ability to measure forces with compact dental arches, it can only determine the maximum occlusal forces. The recorded measurement data do not include information on the dynamics and the loading growth.
From a theoretical point of view, it is possible to distinguish two basic types of design solution for dental dynamometers [14]. The first group includes mechanical dental dynamometers [1]. In this kind of equipment, during the examination, the patients clench their teeth on a dynamometer, with the result that the penetrator leaves the print in the sample, the diameter of which is closely related to the load generated by the muscles responsible for the occluding of dental arches. Inconvenience, resulting from the application, in clinical dentistry, of mechanical dynamometers, is necessary to identify approximating curve factors, as samples prepared in different production cycles may have different mechanical properties. In addition, the material from which the samples are to be taken must meet the following requirements. For example, a copper sample is too hard and is not suitable for the measurement of occlusal forces. However, samples made of lead, due to the high plasticity, can be used effectively only for patients with reduced masticatory organ exercise capacity and patients using mobile dental restorations [15]. The measurement of forces generated by the masticatory muscles with the use of dental mechanical dynamometers, despite their obvious advantages and simplicity of use, also has some drawbacks. Among these should be, above all, the need to precisely measure the diameter of the recess left in the sample by the penetrator. In addition, the undoubted disadvantage of dental mechanical dynamometers is the lack of information on the dynamics of the occlusal forces recorded, as the test result is represented by a numerical value and not by the numbers that change over time.
It is possible to record the nature of change in occlusal forces during clenching by using the electronic force recorder. Analysing the available literature, the development of this type of structure is encountered [16]. The paper attempts to develop a diagnostic measuring device, allowing an assessment of the characteristics of occlusal forces generated under the physiological conditions of chewing. According to the authors [16], a distinctive feature of their solution against the existing design is the ability to dynamically measure the forces in the presence of simulating biting food, placed in any area of natural or artificial teeth. For the measurement of occlusal forces, the authors used a pressure tube sensor connected to the vessel with dimensions 30×10×5 mm, filled with water or saline, which also serves as the simulated biting of food. The sensor, with a specially designed electronic circuit, reads and records continuously the change in the fluid pressure in the vessel. The designed structure of the electronic dental dynamometer, despite the obvious advantages, also has limitations. The range of applications is significantly determined by the size of the tank filled with a liquid, as the geometric dimensions of the tank make it impossible to carry out measurements in the rest position of the mandible, and in this particular position, the muscles responsible for short-circuiting the dental arches generate the largest forces. In work on the evaluation of occlusal forces [17], pressure sensors which were tested on a group of 60 students, were also used, but the presented dental electronic dynamometer allowed only the maximum occlusal forces to be measured.
Taking into account the above limitations of the designed mechanical and electronic dental dynamometer solutions, work was undertaken to develop a new design for the electronic dental dynamometer. In the new solution to the registration of occlusal forces, a thin (about 0.1 mm thickness) piezoresistive FlexiForce sensor made by Tekscan was applied.
2. Materials and methods
The principle of the FlexiForce sensor is the printing of the resistance change of the material on a thin polyester substrate [18]. Typical sensors are made of a thin strip 14 mm wide and 50 to 200 mm long, depending on the destination. At the end of each sensor is a field tester with a diameter of about 10 mm. Important advantages of this type of sensor are their high accuracy, measurement repeatability, and the hysteresis error of less than 3.6 %. In addition, these sensors do not require sophisticated electronics. In the simplest solutions, for the registration of the occlusal forces it is enough to apply a simple multimeter, which allows the resistance to be measured. An increase in pressure on the measurement field causes a change in resistance, which results from a change in the sensor’s terminal voltage. Fig. 1 shows the characteristics of strength and resistance, which are obtained in the range of 0 to 1000 N.
Sensors have different measuring ranges: 4.4 N, 110 N and 440 N. Experimental studies were carried out on the Zwick testing machine, controlled by the TestEkspert computer program, through which it is possible to define complex load cycles. In preliminary measurements, a sensor with a measuring range of up to 440 N was loaded with a force close to 1600 N and, even with such a force so much in excess of the measurement range, the sensor was not damaged. In order to effectively carry out the clinical trials, the r microprocessor force recorder was designed in such a way as to simplify its maintenance as much as possible (Fig. 2).
Fig. 1FlexiForce sensor resistance characteristic 440 N
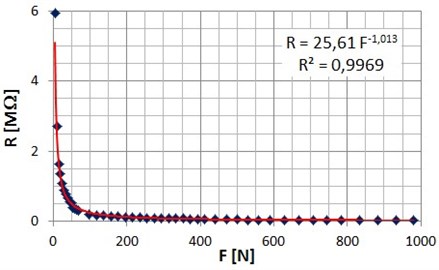
Fig. 2Microprocessor force recorder

When carrying out the measurement of the occlusal forces, the piezoresistive sensor is located between two, thin silver plates, which are placed in a cover made of plastic material inert to body fluids. In addition, the closely fitting cover protects the plates from accidentally falling into the mouth and positions the measuring field relative to the dental arches. The task of the plates is to neutralize the sensory receptors located in the alveolar process, the uniform distribution of pressure on the measurement field of the piezoresistive sensor and protection against damage.
The microprocessor force recorder consists of the meter equipped with an LCD display, a set of connection sockets and control buttons. The device communicates with a PC via a USB port from which it is also powered by 5 V. This voltage does not pose a risk to the patient or to the doctor during the clinical trial. Depending on the adapter and the corresponding head, the designed recorder can handle various kinds of sensors, including strain gauges. It is possible to connect the strain gauges with either a four-wire or six-wire interface. For each type of supported sensor, a dedicated adapter was designed to provide all the necessary connections for the signals and reference voltages. The meter automatically detects the model of adapter used and switches to the appropriate operating mode.
The device is controlled by an AT89C51RD2 microcontroller manufactured by Atmel, whose characteristic feature is its high level performance and rich set of built-in peripheral blocks. The microcontroller firmware is written in assembler, resulting in the optimization of the time spent on the execution of the critical pieces of code. The program stored in the internal ROM of the microcontroller communicates with the user through the input–output devices, which are the control buttons and a backlit LCD. Through the simple on-screen menus, it is possible to select the sampling frequency; the minimum frequency is 7 Hz, while the maximum is 250 Hz. Using a high sampling rate, relatively large text files are created. Recorded signals are affected by noise, which can be significantly reduced with the low sampling frequency. It should be noted that for the measurement of occlusal forces high sampling frequencies are not required, as the loading force on the sensor field increases relatively slowly. The microprocessor force recorder stores the results of clinical trials in the form of graphic images and text files on the PC’s hard drive. To directly determine the size of the occlusal forces, the device is designed in such a way that the measured values are given in Newtons. This effect is achieved by writing the suitable calibration function to the internal memory of the electronic system. The function of the calibration, determined from the synchronized measurement data, was recorded on the test machine and designed dynamometer; wherein the load exerted on the field of the sensor was changed periodically in the range of 0 to 700 N. This range of the load is sufficient to measure the forces, both in the zones of the incisors and the molars.
The first step of the calibration was to eliminate the long-term trend of the voltage time course. In view of the test machine and the microprocessor force recorder recording the force with different frequencies, approximating calibration curves were calculated in the next step.
Approximating curves clearly characterize voltage and force waveforms in the phase of loading and unloading. The use of such a numerical transformation enabled precise synchronization of the two analysed measurement signals. With the analysed time-synchronized signal feet, the voltage-force characteristics were determined on the basis of the searched calibration function. The calibration curve of the piezoresistive sensor was obtained as a result of averaging the characteristics of the phases: loading and unloading of the sensor.
3. Results
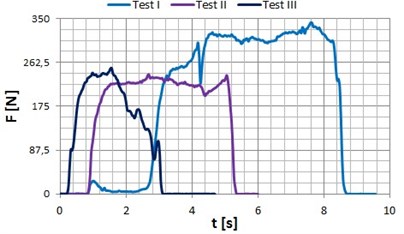
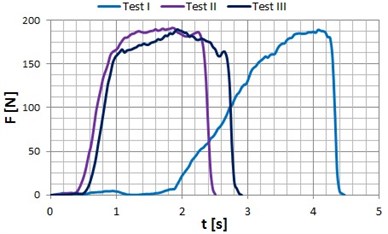
A calibrated measuring transducer was used for clinical testing. Clinical tests were carried out independently in the Medical University of Silesia and the Pomeranian Medical University on four persons with full dental arches who had not complained of problems in the functioning of the stomatognathic system. Below are sample waveforms of occlusal forces that were registered in the area of the teeth: incisors and premolars are shown in the graphs (Fig. 3 to Fig. 6).
Fig. 3Occlusal forces recorded for patient P1 (age: 40 years) in the zone of: a) incisors, b) premolars
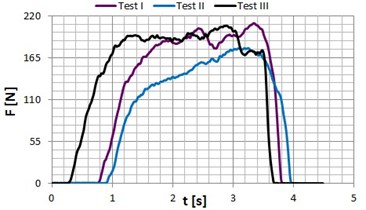
a)
b)
The study of occlusal forces measured by dental mechanical dynamometers shows similar values with measurements obtained using an electronic dental dynamometer. Where the forces recorded by electronic dental dynamometer are slightly larger, this difference can be explained by the fact, that the imprint that arises in a metal sample of a mechanical dynamometer is the result of phenomena associated with the elastic and plastic deformation of the measurement sample.
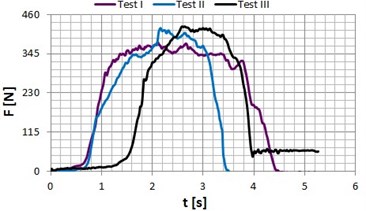
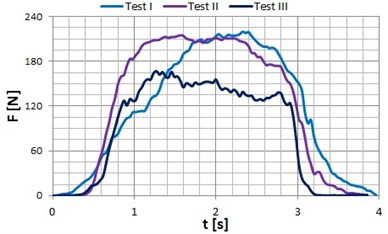
Fig. 4Occlusal forces recorded for patient P2 (age: 22 years) in the zone of: a) incisors, b) premolars
a)
b)
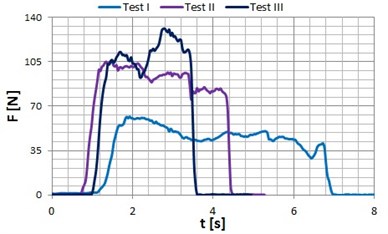
Fig. 5Occlusal forces recorded for patient P3 (age: 23 years) in the zone of: a) incisors, b) premolars
a)
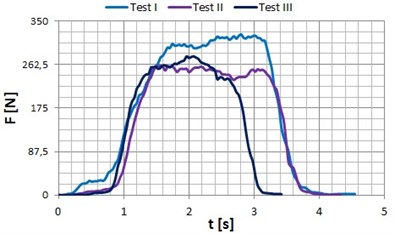
b)
Fig. 6Occlusal forces recorded for patient P4 (age: 24 years) in the zone of: a) incisors, b) premolars
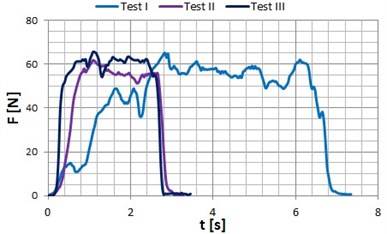
a)
b)
4. Conclusions
The microprocessor force recorder provides for the results of occlusal forces to be given directly in units of the force N, which gives them an objective character. It should be noted that the maximum force exerted on the sensor field depends significantly on the subjective feelings of the patient. Therefore, it is the patient’s decision to discontinue further loading of the sensor field, because the trial should not be a source of discomfort. The electronic dental dynamometer designed and constructed allows not only the actual registration of occlusal forces in the so-called rest position of the jaw, but also forces between the teeth in different phases of dental arch openings. In order to conduct such clinical trials, a specialized measuring head should be used in which a piezoresistive FlexiForce sensor should be mounted.
The main advantage of the microprocessor force recorder of occlusal forces is the continuous-time measurement, and the possibility of carrying out a study of the strength of the masticatory organ muscles. This kind of study is reduced to putting pressure on the measurement area of the sensor for an extended period of time with the maximum force that the patient is able to generate. In the course of this study, with the passage of time, a decrease in occlusal forces was recorded and the time course for the force is the basis for the measurement of fatigue curves. The results of the occlusal forces registered in clinical trials are necessary to carry out modelling studies on the identification of muscle force [19] and the loads acting on the articular discs and temporomandibular joints [14].
References
-
Chladek W. The mechanical modeling of selected states of the human mandible. Scientific Papers of Silesian University of Technology, Metallurgy 59, 2000, (in Polish).
-
Paphangkorakit J., Osborn J. W. Effects on human maximum bite forces of biting on a softer or harder object. Archives of Oral Biology, Vol. 43, Issue 11, 1998, p. 833-839.
-
Chladek W., Lipski T., Karasiński A. Experimental evaluation of occlusal forces. Acta of Bioengineering and Biomechanics, Vol. 3, Issue 1, 2001, p. 25-37.
-
Dýraçoðlu D., Güçlü B., Alptekin K., Karan A., Aksoy C. Maximal bite force measurement by the Istanbul bite force recorder. Journal of Physical Medicine and Rehabilitation Sciences, Vol. 3, 2008, p. 117-123.
-
Calderon P. S., Kogawa E. M., Lauris J. R. P., Conti P. C. R. The influence of gender and bruxism on the human maximum bite force. Journal of Applied Oral Sciencer, Vol. 14, Issue 6, 2006, p. 448-453.
-
Walimoto A., Könönen M. A novel bite force recorder and maximal isometric bite force values for healthy young adult. Scandinavian Journal of Dental Research, Vol. 101, Issue 3, 1993, p. 171-175.
-
Singh S., Utreja A. K., Sandhu N., Dhaliwal Y. S. An Innovative miniature bite force recorder. International Journal of Clinical Pediatric Dentistry, Vol. 4, Issue 2, 2011, p. 113-118.
-
Sathyanarayana H. P., Premkumar S. Assessment of maximum voluntary bite force in children and adults with normal occlusion. International Journal of Pharmaceutical Science and Health Care, Vol. 2, Issue 1, 2012, p. 64-70.
-
Krzemień J., Baron S. Axiographic and clinical assessment of temporomandibular joint function in patients with partial edentulism. Acta of Bioengineering and Biomechanics, Vol. 15, Issue 1, 2013, p. 19-26.
-
Margielewicz J., Chladek W., Lipski T. Kinematical analysis of mandibular motion in the sagittal plane. Acta of Bioengineering and Biomechanics, Vol. 10, Issue 1, 2008, p. 9-19.
-
Gąska D., Kijak E., Lipski T., Margielewicz J. Numerical modelling of human masticatory organ kinematics. Mechanika, Vol. 18, Issue 4, 2012, p. 447-452.
-
Wojnarowski J., Kijak E., Gąska D., Margielewicz J. Research model of stomatognathic system’s kinematics in protrusive movement. International Journal of Applied Mechanicics and Engineering, Vol. 17, Issue 3, 2012, p. 1051-1059.
-
Kim B. I., Jeong S. H., Chung K. H., Cho Y. K., Kwon H. K., Choi C. H. Subjective food intake ability in relation to maximal bite force among Korean adults. Journal of Oral Rehabilitation, Vol. 36, 2009, p. 168-175.
-
Margielewicz J., Kijak E., Lipski T., Pihut M., Kosiewicz J., Lietz-Kijak D. Biostatic equilibrium model study of human masticatory system. Center for Biomedical Engineering of Silesian University of Technology, Gliwice, Vol. 203, 2012, (in Polish).
-
Lipski T. Influence of selected characteristics of oral forces to maintain the full lower denture with alveolar bone loss. Katowice, 2005, (in Polish).
-
Kociubiński A., Duk M., Zyska T., Michalski W. Sensor measuring system for the treatment of bite force evaluation of masticatory efficiency. Electrical Review, Vol. 86, Issue 20, 2010, p. 50-52, (in Polish).
-
Abu Alhaija E. S. J., Al Zo’ubi I. A., Al Rousan M. E., Hammad M. M. Maximum occlusal bite forces in Jordanian individuals with different dentofacial vertical skeletal patterns. European Journal of Orthodontics, Vol. 32, 2010, p. 71-77.
-
Sarzyński A. Measurements of pressure forces – flexible FlexiForce sensors. Practical Electronics, Vol. 3, 2010, p. 134-137, (in Polish).
-
Wojnarowski J., Margielewicz J., Chladek W. Modelling studies as a tool for the identification of masticatory muscle strength. Acta Mechanica et Automatica, Vol. 4, Issue 3, 2010, p. 138-142, (in Polish).
About this article

