Abstract
The purpose of this review document is to summarize the latest developments and research in the field of robotics related to the field of ankle joint rehabilitation, review new results, and determine the actual state of the art. The literature search was carried out using scientific and medical databases and other websites related to robots used in the field of ankle rehabilitation, analyzing research from the 1950s to the present.
Highlights
- Today, the main problems in the field of robot rehabilitation are the lack of unique rehabilitation programs that can meet the needs of all types of patients, and the lack of additional resources to measure the effectiveness of yet-to-be-commercialized robots.
- To date, the main problems in the field of robotic rehabilitation are the lack of unique rehabilitation protocols that can meet the needs of all types of patients, and additional resources to evaluate the effectiveness of proposals that have not yet been commercialized.
- This article provided an overview of research and recommendations on robotics for ankle rehabilitation. The biomechanics of the ankle joint is based on axes and planes of motion; joint movements have been briefly described. Several variants of rehabilitation robots were considered, which were classified according to such features as construction and design.
1. Introduction
The human ankle joint is a very complex structure of the human skeleton and plays an important role in the transmission of forces and moments when moving [1]. There are many factors that can lead to a violation of the function of the ankle joint or a restriction of the range of movement performed in everyday life. The ankle joint is one of the most traumatic joints in the human body due to excess weight, excessive physical activity, or its lack, for example, congenital pathologies that occur in the elderly. The most common damage to the ankle joint is stretching of the ligaments of the joint. They occur when the joint performs excessive functional movements, for example, in athletes, and can also occur in people who perform passive movements, that is, lead a mostly sedentary lifestyle [2]. Weakness of the lower extremities, i.e., inability to lift the head and toes of the feet, is another manifestation of damage (disability) of the lower leg and foot joints. There are also neurological disorders caused by bone fractures or strokes and spinal injuries, paralysis, hemiparesis, etc. other serious diseases, such as ankle rehabilitation, make it a much longer and more complex process. The types of physiotherapy procedures used to restore the ankle joint vary and depend on the specific condition of the patient’s muscles or skeleton. Strengthening and resistive exercises are usually recommended. Among the exercises most often prescribed to patients are passive, auxiliary and active exercises. Unlike other passive exercises, the patient does not make any effort when performing the exercise. Instead, a physical therapist helps patients move, move, and maintain their leg muscles and joints. An auxiliary type of exercise is an intermediate method that combines the efforts of the patient and the physiotherapists, i.e., passive exercises are performed in parallel with active exercises. In active training, the patient himself makes physical efforts. And during the last resistive exercises, special mechanical devices are used to counteract the patient, that is, the patient faces obstacles while moving.
The main requirement that patients are asked to achieve a successful result in any rehabilitation work is to perform it intensively, without interrupting the training program. The frequency and duration of such programs depends on the patient's condition, ability to move. However, if the patient does not have time or is limited from the program due to the state of funds, his chances of recovery decrease. In addition, many exercises can be repeated many times, and a lot of work is done with the physical therapist, so the patient's emotional and physical efforts can be exhausted over time. The equipment needed to restore the ankle joint, whether it is a rehabilitation center or at home, is quite simple.
Interest in overcoming the shortcomings of traditional systems, in the design and development of automatic equipment for physiotherapy has increased. The use of robots in rehabilitation therapy has many advantages: (a) various exercises can be performed using a unique device; (b) robots provide computerized information useful for accurate diagnosis, monitoring the rehabilitation process and individual therapy; (c) robots can perform intensive exercises that accelerate the patient's recovery without interfering with the therapist [2].
This paper provides an overview of the latest modern achievements and research in the field of robotics related to the rehabilitation of the ankle joint. The content of the work is organized as follows: First, a brief description of the biomechanics of the ankle joint is given. In the second part, platform robots are used in the process of rehabilitation of the human ankle joint. And the robot architectures and commercial robots and their most popular modern prototypes will be compared. The fourth section discusses the most important issues of rehabilitation work of the ankle joint with robots: (a) robot design, (b) user interface, (c) control and control. At the end of the work, several conclusions are drawn on the research.
2. Biomechanics of the ankle joint
To design and create robots, it is very important to know the biomechanics of the ankle joint. It will help you choose the robot parameters needed to prepare the design of rehabilitation robots that are effective for patients with impaired motor function, such as walking, and will not damage them. The legs are the main part of the human musculoskeletal system, and they can simultaneously have rigid and flexible structures due to various motor features. The anatomical structure of the ankle joint is very complex and consists of the following parts: 4 bones, 7 muscles, 9 tendons, and 4 groups of ligaments.
As shown in Fig. 1(a), the combination of the tibia and subtitle joints facilitates movement in the ankle joint [3]. The tibia joint forms a connection between the tibia and the fibula and the upper surface of the talus bone, while the subtitle joint forms a connection between the lower part of the talus bone and the upper surface of the heel bone. Fig. 1(b) shows the axes of rotation of the ankle joint relative to the tibia and subtitle joints.
Fig. 1a) Ankle joint, b) planes and movements of the ankle joint
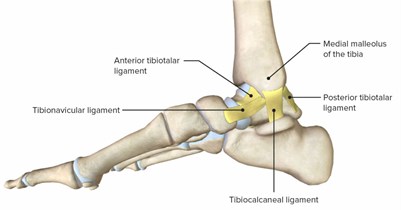
a)
b)
Axes and planes of rotation are used to characterize the spatial configuration of the ankle joint. The foot can be considered divided into sagittal, frontal, and transverse planes (Fig. 1(a)). These planes allow us to find three axes of rotation in the mutual pediculus used to design the movement of the joint (parallel to these planes) [4]. Using both axes and planes, movements in the joints can be classified as follows: (a) bending of the sole outward and inward – they are characterized by movements around the axis formed by the mutual intersection of the sagittal and transverse planes, in the sagittal plane. Bending the sole outward is a type of movement that is performed by bending the sole upwards, that is, towards the Shin, so that the angle between the lower leg and the sole is less than 90 degrees. Movement against it-the foot bends down at an angle of more than 90 degrees from the ankle; (b) eversion and inversion movements are movements parallel to the frontal plane. An eversion motion is a lateral flexion of the sole, and an inversion is a medial flexion; (c) abduction and adduction are rotational movements of the heel around its axis parallel to the horizontal plane. Abduction is a lateral displacement of the forelimbs, and adduction is a medial displacement.
Supination and pronation are complex movements that consist of a combination of the three movements mentioned above. Supination combines inversion movement, downward flexion of the sole, and adduction movement. And pronation is a combination of eversion, upward flexion of the foot, and abdication movements (Fig. 1(b)) [5]. The study of the mobility of the ankle joint begins primarily with determining only the range of movement [6, 7].
3. Classification of ankle rehabilitation robots
Robots for rehabilitation of the ankle joint can be divided into two groups: active orthoses or exoskeleton robots and platform robots. The architectural features of platform robots are considered.
4. Platform robots
Platform robots, unlike exoskeletal robots and mechanical prostheses, are stationary. To apply force to the leg and move it, the patient puts his foot on a sliding platform. Such robots have a different architecture that allows robots to perform complex and special spatial movements, and they have no weight restrictions such as exoskeletons and orthoses. Platform robots usually use parallel mechanisms, including kinetic chains between a fixed platform and a mobile platform. The high rigidity gives this device a uniformly distributed force [8]. They are usually designed to perform movements such as inversion-inversion and bending the sole up and down. They are aimed at the rehabilitation of patients with impaired limb movement or low mobility, including the improvement of motor skills and proprioception of the patient's ankle joint. However, they have the following disadvantages:
1) unnatural proprioception of the patient caused by the difficulty of identifying the axes of rotation of the platform on which the foot is located and the axes of rotation of the natural ankle joint of a person.
2) chem is less used in motion rehabilitation exercises because it is not small.
3) even though the device has an effective and high ability to perform tasks such as collecting information, generating reports, and assessing the patient's condition, it can only be managed by a specialist, so it is only available for use in a clinical setting and the price is very high.
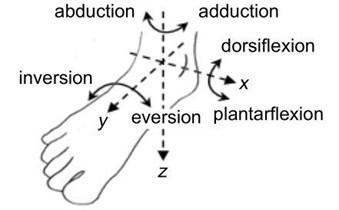
The emergence of such robotic devices was stimulated by the emergence of parallel platform robots invented by Goff-Stewart in 1965 [9]. One of the most popular first robots in this category is the Rutgers Ankle robot [10]. It allows you to move with six degrees of freedom controlled by pneumatic Pistons and develop a rehabilitation program based on weight training. The Rutgers Ankle robot opened the way for the therapist to remotely control the patient, which was very useful for treating diseases such as stroke and tendon sprain. These robots have been clinically studied and can be found in some scientific literature [11]. However, this mechanism is not widely used in rehabilitation therapies (Fig. 2(а) shows the appearance of the robot).
Yun et al. investigated the possibility of performing relative rotational and direct movements between platforms using a platform robot of the 2-PSPP+PRR type with pneumatic drive [15]. In addition, it was proposed to reconfigure the platform robots relatively, due to the long platform, these robots made it possible not only to perform stretching exercises, but also to perform balance and proprioception movements. The 3-UPS, invented by Lee and Shah, improved the structure of the platform robot, and was used to simulate the movement of the two-axis ankle joint [16].
Homma and others proposed a platform robot that allows you to perform inversion-eversion passive movements when the sole is bent up and down [17]. Tsoi and Chi proposed a 4-UPS suspension robot design, the advantage of which is that it provides adjustment of the vertical reaction force, so that the robot can be adapted to different patients with a small modification of its design [18]. Lin and others have developed a convenient robot prototype that combines three passive, active and resistive methods of restoring gait. This freedom allowed us to solve some of the problems of degree, muscle strength, and proprioception [19].
Fig. 2a) Rutgers Ankle platform robot, b) platform robot prototype presented by Yun et al
a)
b)
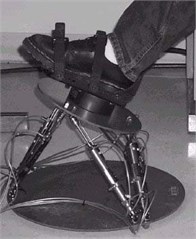
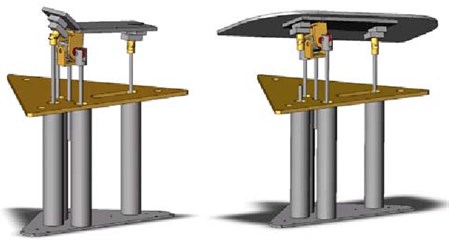
After the appearance of robots with which it was possible to make auxiliary movements with high sensitivity, Ordo and others presented a new original robot prototype, in which the action of the electric motor on one side of the joint is directly related to the sensors that collect information on the opposite side of the Joint [20]. They recommend connecting tendons to work by vibrating during arbitrary contractions to improve tendon stretches and proprioception after a stroke. Salya, etc. ARBOT introduced a prototype robot called 3-UPS+U, which allows you to perform movements such as up-down flexion of the foot, inversion-eversion, and displacement of the lower leg outward and inward [21]. It also combines a foot position control system and a remote-control system for active and resistive exercises when performing slow exercises [22]. Jamwal and others proposed a prototype of a soft parallel robot, the mechanism of which combines the work of pneumatic muscles and a magnetorheological drive [23]. Dean and others developed the Nuvabat robot, which provides variable torque, force measurement, and data collection to determine the pressure center [24]. Nuvabat, like tebibit robots, provides a virtual reality environment for performing a training program [25].
Fig. 3a) Robots made by Jamwal, b) JACE Ankle A330 CPM robot prototype
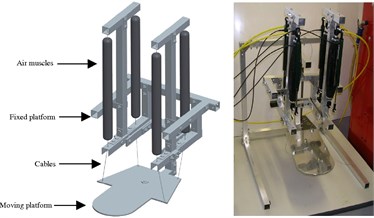
a)

b)
In recent years, interesting new robot architectures have appeared: Sung et al. [25] modified the robot mechanism with four elastic rods that allow you to adjust the volume of movement when the sole bends up and down. Wang and others proposed a parallel robot design with three degrees of freedom of Type 3-RUS/RRR. They can create an axis of rotation of the joints and can distinguish between movements with two degrees of freedom associated with rehabilitation training. Zhou, etc. [26] developed a prototype platform robot that was used to treat muscle tension and passed clinical trials. There are several commercial platform robots that are used for the rehabilitation of the ankle joint: as an example, we can mention the Kinetic robots offered by Breva for adults and 5090 for children [27]. This robot, proposed by Breva, has two degrees of freedom, so it can use it to perform both bending and inversion-eversion movements of the foot up and down. And since the prototype robot 5090 allows you to shift the lower leg to the limit, it is recommended to use it, especially for joint stiffness and non-spastic paralysis in children. The OptiFlex [28] robot from Chatamoog consists of two degrees of freedom, so its patented design allows you to perform bending of the sole up and down and inversion-eversion movements.
JACE Ankle A330 CPM [29] is a robot with a single degree of freedom and is designed for use when the tendons of the ankle joint are stretched. Biodex Multi-Joint System 4 Pro is another complex structured and affordable robot [27]. It is designed for the rehabilitation of not only the ankle joint, but also many other joints (Fig. 3(b)).
5. Overview of robot development issues
In the previous sections, we discussed a wide range of robotic systems for rehabilitation of the ankle joint, but only a small part of them is commercialized. There are some non-commercial robots that are still at the stage of modeling and experimental testing. Commercialization is limited by many factors; however, the most important factor is the lack of standardized evaluation criteria that assess the effectiveness of robots for ankle rehabilitation. In addition, there is no final rehabilitation program for the treatment of patients. This means that it is necessary to identify and develop the most effective treatment program. This makes it difficult to decide what tasks to perform when creating robots.
Although research and development in this area has expanded significantly in recent decades, there are several issues that need to be addressed in terms of the performance, safety, and versatility of the robotic system. Based on the basic principles of the design of rehabilitation robots, it is possible to distinguish current issues in terms of the design, interface, and automation of the management of the rehabilitation robot.
6. Design of a rehabilitation robot and its design
Creating a rehabilitation robot design is a difficult task. First, it is an extremely difficult process to accurately simulate various ankle movements. The position of the two joints that provide movement of the ankle in comparison with each other varies from person to person, and when walking, their axes of rotation move relative to each other. Thus, the robot must have a structure that adapts to each patient. Many robots serve as auxiliary support devices for the patient's training during the rehabilitation process, but they are not comparable to the therapist in their flexibility and responsiveness. This is mainly since the mobility, accuracy and reaction time of robotic systems are negatively affected by the weight and size of the devices.
One of the last requirements for the design of the robot is that when the device interacts with the patient, the patient’s safety must be considered.
Another important feature of the design of rehabilitation robots is the interface, which receives feedback from both the therapist and the patient. The relationship between the patient and the robot is one of the most important issues in the development of robotic rehabilitation devices, but these recommendations are practically not considered in the development and recommendations of the robot.
Studies have shown that human perception of robots largely depends on the appearance of the robot. Some authors explain that the more functional robots look for adults, the better they are perceived. However, there is little literature on this issue. The necessary goal in designing robots, of course, in addition to helping the therapist, is to provide the patient with comfort. At the same time, for the successful implementation of rehabilitation therapy, the patient needs to be satisfied with the robot.
Currently, among the robotic systems mentioned earlier, only a few use a virtual reality interface. Visual imitation of the patient himself and his movements is one of the ways robots adapt to different users of different ages and lifestyles and is considered as a separate area of research.
7. Conclusions
In this paper, an overview of research and recommendations on robotics for the rehabilitation of the ankle joint was presented. Biomechanics of the ankle joint based on axes and planes of movement; joint movements were briefly described. Several variants of rehabilitation robots were considered, which were classified according to such features as construction and design. To date, the main problems in the field of robot rehabilitation are the lack of unique rehabilitation protocols that can meet the needs of all types of patients, and additional resources to evaluate the effectiveness of proposals that have not yet been commercialized. However, we have mentioned above three areas where design issues are more relevant. The first of them is the robot architecture, which currently still creates some difficulties to simulate the natural movement of the ankle joint. Thus, the displacements experienced by the axes in the joint must be adapted to each patient and a wide range of pathologies. Moreover, many proposals were not conceived for the purpose of commercialization, and even more so to become an object of personal use.
References
-
Jiacong W., “Rehabilitation of ankle and foot,” Chinese Journal of Rehabilitation Theory and Practice, pp. 1197–1198, 2008.
-
Y. M. Khalid, D. Gouwanda, and S. Parasuraman, “A review on the mechanical design elements of ankle rehabilitation robot,” Proceedings of the Institution of Mechanical Engineers, Part H: Journal of Engineering in Medicine, Vol. 229, No. 6, pp. 452–463, Jun. 2015, https://doi.org/10.1177/0954411915585597
-
S. Siegler, J. Chen, and C. D. Schneck, “The three-dimensional kinematics and flexibility characteristics of the human ankle and subtalar joints-part I: kinematics,” Journal of Biomechanical Engineering, Vol. 110, No. 4, pp. 364–373, Nov. 1988, https://doi.org/10.1115/1.3108455
-
M. Malosio, S. P. Negri, N. Pedrocchi, F. Vicentini, M. Caimmi, and L. Molinari Tosatti, “A spherical parallel three degrees-of-freedom robot for ankle-foot neuro-rehabilitation,” in 2012 34th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), pp. 3356–3359, Aug. 2012, https://doi.org/10.1109/embc.2012.6346684
-
“Motions of the foot and ankle.”. http://www.northcoastfootcare.com/
-
J. T. Manter, “Movements of the subtalar and transverse tarsal joints,” Anatomical Record, Vol. 80, No. 4, pp. 397–410, 1941.
-
Barnett Ch and Napier Jr, “The axis of rotation at the ankle joint in man; its influence upon the form of the talus and the mobility of the fibula,” Journal of anatomy, Vol. 86, No. 1, pp. 1–9, Jan. 1952.
-
C. E. Syrseloudis and I. Z. Emiris, “A parallel robot for ankle rehabilitation-evaluation and its design specifications,” in 2008 8th IEEE International Conference on Bioinformatics and BioEngineering (BIBE), pp. 1–6, Oct. 2008, https://doi.org/10.1109/bibe.2008.4696826
-
B. Dasgupta and T. S. Mruthyunjaya, “The Stewart platform manipulator: a review,” Mechanism and Machine Theory, Vol. 35, No. 1, pp. 15–40, Jan. 2000, https://doi.org/10.1016/s0094-114x(99)00006-3
-
M. J. Girone, G. C. Burdea, and M. Bouzit, “The “Rutgers Ankle” orthopedic rehabilitation interface,” in ASME 1999 International Mechanical Engineering Congress and Exposition, p. 1999, Nov. 1999, https://doi.org/10.1115/imece1999-0040
-
M. Zhang, T. Davies, and S. Xie, “Effectiveness of robot-assisted therapy on ankle rehabilitation – A systematic review,” Journal of NeuroEngineering and Rehabilitation, Vol. 10, No. 1, p. 30, 2013, https://doi.org/10.1186/1743-0003-10-30
-
Hicks J., “The mechanics of the foot. I. The joints.,” Journal of Anatomy, Vol. 87, pp. :345–357, 1953.
-
F. Gholami, R. Pàmies-Vilà, J. Kövecses, and J. M. Font-Llagunes, “Effects of foot modelling on the human ankle kinematics and dynamics,” Mechanism and Machine Theory, Vol. 93, pp. 175–184, Nov. 2015, https://doi.org/10.1016/j.mechmachtheory.2015.07.003
-
G. Liu, J. Gao, H. Yue, X. Zhang, and G. Lu, “Design and kinematics analysis of parallel robots for ankle rehabilitation,” in 2006 IEEE/RSJ International Conference on Intelligent Robots and Systems, Vol. 446-447, pp. 1279–1284, Oct. 2006, https://doi.org/10.1109/iros.2006.281710
-
J. Yoon, J. Ryu, and K.-B. Lim, “Reconfigurable ankle rehabilitation robot for various exercises,” Journal of Robotic Systems, Vol. 22, No. S1, pp. S15–S33, Sep. 2006, https://doi.org/10.1002/rob.20150
-
K.-M. Lee and D. K. Shah, “Kinematic analysis of a three-degrees-of-freedom in-parallel actuated manipulator,” IEEE Journal on Robotics and Automation, Vol. 4, No. 3, pp. 354–360, Jun. 1988, https://doi.org/10.1109/56.796
-
K. Homma and M. Usuba, “Development of ankle dorsiflexion/plantarflexion exercise device with passive mechanical joint,” in 2007 IEEE 10th International Conference on Rehabilitation Robotics, pp. 292–297, Jun. 2007, https://doi.org/10.1109/icorr.2007.4428440
-
Y. H. Tsoi and S. Q. Xie, “Design and control of a parallel robot for ankle rehabiltation,” in 2008 15th International Conference on Mechatronics and Machine Vision in Practice (M2VIP), pp. 515–520, Dec. 2008, https://doi.org/10.1109/mmvip.2008.4749585
-
Chou-Ching K. Lin, Ming-Shaung Ju, Shu-Min Chen, and Bo-Wei Pan, “A specialized robot for ankle rehabilitation and evaluation,” Journal of Medical and Biological Engineering, Vol. 28, No. 2, pp. 79–86, Jun. 2008.
-
P. Cordo, H. Lutsep, L. Cordo, W. G. Wright, T. Cacciatore, and R. Skoss, “Assisted movement with enhanced sensation (AMES): coupling motor and sensory to remediate motor deficits in chronic stroke patients,” Neurorehabilitation and Neural Repair, Vol. 23, No. 1, pp. 67–77, Jan. 2009, https://doi.org/10.1177/1545968308317437
-
J. A. Saglia, N. G. Tsagarakis, J. S. Dai, and D. G. Caldwell, “A high performance 2-dof over-actuated parallel mechanism for ankle rehabilitation,” in 2009 IEEE International Conference on Robotics and Automation (ICRA), May 2009, https://doi.org/10.1109/robot.2009.5152604
-
J. A. Saglia, N. G. Tsagarakis, J. S. Dai, and D. G. Caldwell, “Control Strategies for Patient-Assisted Training Using the Ankle Rehabilitation Robot (ARBOT),” IEEE/ASME Transactions on Mechatronics, Vol. 18, No. 6, pp. 1799–1808, Dec. 2013, https://doi.org/10.1109/tmech.2012.2214228
-
P. K. Jamwal, S. Xie, and K. C. Aw, “Kinematic design optimization of a parallel ankle rehabilitation robot using modified genetic algorithm,” Robotics and Autonomous Systems, Vol. 57, No. 10, pp. 1018–1027, Oct. 2009, https://doi.org/10.1016/j.robot.2009.07.017
-
Ye Ding, M. Sivak, B. Weinberg, C. Mavroidis, and M. K. Holden, “NUVABAT: Northeastern university virtual ankle and balance trainer,” in 2010 IEEE Haptics Symposium (Formerly known as Symposium on Haptic Interfaces for Virtual Environment and Teleoperator Systems), Mar. 2010, https://doi.org/10.1109/haptic.2010.5444608
-
E. Sung, A. H. Slocum, R. Ma, J. F. Bean, and M. L. Culpepper, “Design of an ankle rehabilitation device using compliant mechanisms,” Journal of Medical Devices, Vol. 5, No. 1, p. 01100, Mar. 2011, https://doi.org/10.1115/1.4002901
-
Z. Zhou, Y. Zhou, N. Wang, F. Gao, K. Wei, and Q. Wang, “A proprioceptive neuromuscular facilitation integrated robotic ankle-foot system for post stroke rehabilitation,” Robotics and Autonomous Systems, Vol. 73, pp. 111–122, Nov. 2015, https://doi.org/10.1016/j.robot.2014.09.023
-
“Biodex.”. https://www.biodex.com/physical-medicine/products/dynamometers/system-4-pro
-
C. Gosselin and Jean-François Hamel, “The agile eye: a high-performance three-degree-of-freedom camera-orienting device,” in Proceedings of the 1994 IEEE International Conference on Robotics and Automation, pp. 781–786, 1994, https://doi.org/10.1109/robot.1994.351393
-
Simnofske M. et al., “Active ankle-an almost spherical parallel mechanism,” in Proceedings of ISR 2016: 47st International Symposium on Robotics, 2016.
Cited by
About this article

