Abstract
Satisfactory chewing is performed by an alternating bilateral pattern that depends on occlusal balance, the absence of occlusal interference or premature contacts, stability, good functioning of the temporomandibular joints (TMJs) and neuromuscular maturation. If mandibular functional imbalances occur, discrepancies in maxillomandibular development and future facial asymmetries may occur. The objective of this work was to remove dental interferences that cause anterior and posterior crossbite, as well as those that prevent the good execution of symmetrical lateroprotrusive movements (right side/left side), through occlusal adjustment and subsequent correction of maxillary asymmetry using the device; encapsulated. Clinical case report of a two-year-old female patient, with unilateral crossbite on the right side (anterior/posterior), diagnosed with congenital torticollis, difficulty breastfeeding and difficulty performing alternating lateral movements. with follow-up until the complete deciduous dentition. The treatment was divided into three stages. The first step was to correct the unilateral crossbite (anterior and posterior), on the right side, by making occlusal adjustment using a grid, and later with the addition of Planas Direct Tracks resin. The second stage used an encapsulated device to correct maxillary asymmetry. The third stage was completed after the eruption of the deciduous second molars with the functional analysis of lateral movements plus occlusal adjustments using a grid. Correction of unilateral crossbite (anterior and posterior) on the right side, symmetrization of the maxilla and better execution of lateroprotrusive movements. The results obtained in this case report suggest that the occlusal adjustment removed the dental interferences that caused the anterior/posterior crossbite on the right side; the maxilla was symmetrized with the distalization of sector 63-65, and the removal of dental interferences that prevented lateral movements made it possible to perform lateroprotrusive movements (right/left side) after the complete eruption of the primary teeth.
1. Introduction
Satisfactory chewing is achieved by a bilateral alternating pattern, absence of occlusal interferences or premature contacts, stability, good functioning of the temporomandibular muscles (TMJ), neuromuscular maturation and symmetry of the maxilla, since skeletal asymmetries at the base of the skull can make correct chewing difficult [1, 2].
At approximately 6 years of age, the construction of the base of the face has practically been completed. The symmetrical development of the skull bones is essential so that the mandible can perform lateral-protrusive movements bilaterally. The maxilla is anatomically connected to the frontal, ethmoid and sphenoid bones; concomitantly, the mandible, through the condyle, articulates with the mandibular fossa inserted into the temporal bones. Any change in the bones at the base of the skull can impact mandibular positioning [2-4].
It is known that a greater number of dental contacts when carrying out chewing movements leads to more effective chewing [4]. Any situation that alters the development of the skull base, such as congenital torticollis, for example, needs to be investigated in a timely manner and directed to specific professionals; physiotherapists.
Congenital torticollis is characterized by shortening of the sternocleidomastoid muscle (SCM), limiting movement of the neck, which is quite evident at birth or after birth. Hypomobility of the neck promotes cervical flexion on the affected side and cervical rotation on the opposite side, leaving the baby predisposed to developing flattening of the occipital bone. If the tension pattern is maintained, the flattening may progress to positional plagiocephaly [3, 5-7]. Positional plagiocephaly can anteriorize the position of the mandibular fossa and condyle on this side, leading the baby to develop a tilt of the jaw on the opposite side, with early approximation between the dental arches on this side, predisposing to the development of unilateral crossbite [6, 7].
The baby may have difficulty sucking both breasts or hurt one breast; The vacuum of the tongue may be compromised due to the change in position of the jaw, making suction ineffective, which may make chewing difficult in the future [1, 6, 8].
For correct chewing development, the vertical dimensions on both sides must be symmetrical. It is recommended that if there are different vertical dimensions, the chewing function will occur more frequently where this vertical dimension is smaller, as the mandible will need to unclude less, generating less energy expenditure in the chewing process [9]. If the altered function remains, over time it may lead to discrepancies in maxillomandibular development and future facial asymmetries [9, 10].
The present work aims to remove both dental interferences that cause anterior and posterior crossbite, as well as those that prevent latero-protrusive movements from being well executed (right/left side) [9], [10], through symmetrization of the maxilla and occlusal adjustments.
2. Methodology
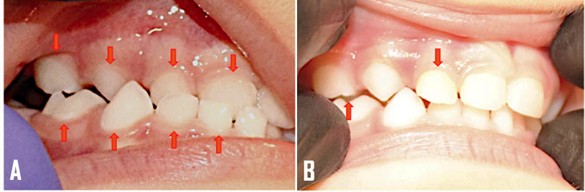
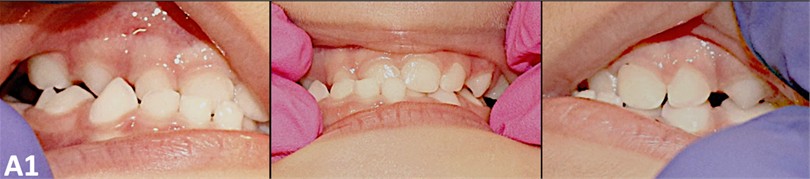
Clinical case report of a two-year-old female patient, with unilateral crossbite on the right (anterior/posterio) (Fig. 1), diagnosed with congenital torticollis, difficulty breastfeeding and difficulty performing alternating lateral movements. The treatment was divided into three stages: the first stage consisted of occlusal adjustment without the eruption of the deciduous second molars. The second stage began with the complete eruption of all primary teeth and was completed after 7 months. The third step was performed after removing the device.
Fig. 1Patient with unilateral right anterior/posterior crossbite

Fig. 21st stage: Occlusal adjustment by grid and addition of resin. In A, Grid was performed on the palatal surface of teeth 51/52/53; palatal cusp of tooth 54 and buccal surface of teeth 81/82/83/84. In B, addition of resin was carried out on the lingual cusp of tooth 84 and Inclined Plane on the buccal surface of tooth 52
1st Stage: Occlusal adjustment by adding resin to the posterior teeth with Planas Direct Tracks. Occlusal adjustments were performed on the right unilateral anterior side and the posterior crossbite side. Grid was performed on the palatal surface of teeth 51/52/53; palatal cusp of tooth 54 and buccal surface of teeth 81/82/83/84. The addition of resin was carried out on the lingual cusp of tooth 84 and Inclined Plane on the buccal surface of tooth 52. Flat Direct Tracks were placed only on primary teeth that presented dental interference (Fig. 2).
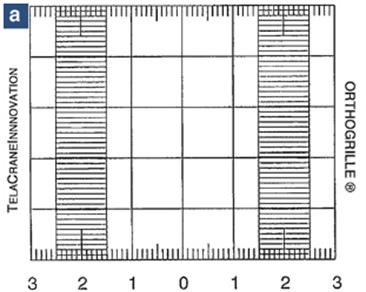
2nd Stage: Symmetrization of the maxilla. To detect maxillary asymmetry, the Orthogrille ®instrument was used (Fig. 3).
Fig. 3Orthogrille image®
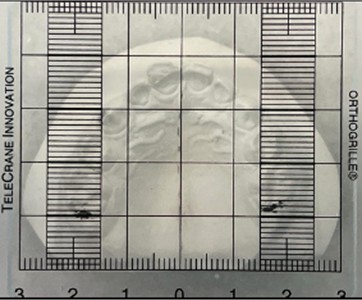
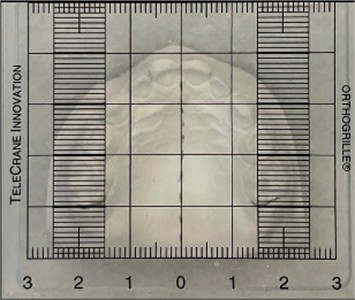
The Orthogrille® was positioned on the cut plaster model. A dotted line was drawn in the region of the palatal raphe to the most distal point of the incisive papilla and around the lingual surface of the second molars (Fig. 4). The Othogrille was used to measure the symmetry of the maxilla and an intra-arch sagittal asymmetry was detected, where the left hemi-maxilla was more mesialized than the right.
Fig. 4A dotted line was drawn in the region of the palatal raphe to the most distal point of the incisive papilla and around the lingual surface of the second molars
An encapsulated device based on devices by Maurício [13] and Deshayes [2] was installed with the purpose of distalizing sector 63-65 of the left hemi-maxilla and repositioning the mandible (Fig. 5). This device is a functional orthopedic device as it promotes changes in posture and therapeutic posture through adjustments to the device’s acrylic to enable mandibular movement.
The treatment to correct asymmetry lasted 7 months, with device activations every 15 days (Fig. 6).
Fig. 5Image of the encapsulated device based on devices from Maurício [ 13] and Deshayes [2]
![Image of the encapsulated device based on devices from Maurício [ 13] and Deshayes [2]](https://static-01.extrica.com/articles/24353/24353-img5.jpg)
Fig. 6Hemi-maxilla with corrected distalized sector 63-65
3rd Step: Occlusal Adjustment by grid (Fig. 7). After symmetrization of the maxilla, occlusal adjustment was performed using a grid on the mesial surface of teeth 53/63 and on the distal surface of teeth 73/83, enabling the mandible to perform ideal chewing.
Fig. 73rd stage: Occlusal adjustment by grid. The criteria for occlusal adjustments by grid were based on mandibular dynamics (opening/closing, right and left laterality and protrusion movements). The grid was performed on the mesial side of teeth 53/63 and on the distal side of teeth 73/83

3. Results
Fig. 8 presents the three completed steps. In Fig. 8(a) we can observe the anterior/posterior crossbite on the right side and in Fig. 8(b) the correction of this anteroposterior crossbite with occlusal adjustment by grid on the palatal surface of teeth 51/52/53, palatal cusp of tooth 54, and buccal surface of teeth 81/82/83/84 and addition of resin with Planas Direct Tracks on the lingual surface of the buccal cusp of tooth 84 and buccal surface of tooth 52. In Fig. 8(c), encapsulated device based on devices by Maurício [13] and Deshayes [2] it was installed with the purpose of distalizing sector 63-65 of the left hemi-maxilla and repositioning the mandible. In Fig. 8(d), after 7 months, there was correction of the distalization of sector 63-65 and the execution of lateroprotrusive movements after occlusal adjustment by g rad and the mesial surface of teeth 53/63 and the distal surface of teeth 73/83.
Fig. 8The three completed steps
a) Anterior/posterior crossbite on the right side

b) Correction of anteroposterior crossbite with occlusal adjustment using a grid on the palatal surface of teeth 51/52/53, palatal cusp of tooth 54 and buccal surface of teeth 81/82/83/84, and addition of resin with Planas Direct Tracks on the lingual surface of the buccal cusp of tooth 84 and Inclined Plane on tooth 52

c) Installation of the encapsulated device with the purpose of distalizing sector 63-65 of the left hemi-maxilla and repositioning the mandible

d) After 7 months, the distalization of sector 63-65 was corrected and lateroprotrusive movements were performed after occlusal adjustment by grid of the mesial surface of teeth 53/63 and the distal surface of teeth 73/83
4. Discussion
The treatment was carried out in a timely manner as a crossbite will have repercussions on the development and growth of the stomatognathic system [4].
Changes in the bones at the base of the skull can alter mandibular positioning [2]. The dental interference that caused the corrected crossbite, followed by the symmetrization of the maxilla and the occlusal adjustment may impact harmonious mandibular movements.
5. Conclusions
Functional Jaw Orthopedics restores bilateral and alternate mandibular movements, so that the patient can perform ideal chewing. Dental interference occurs due to the underdevelopment of the stomatognathic system, facilitating the installation of the crossbite. The crossbite was corrected, the maxilla was symmetrized with the distalization of sector 63-65 and the removal of dental interference made it possible to perform lateroprotrusive movements (right/left side).
References
-
C. W. Genna, “Breastfeeding infants with congenital torticollis,” Journal of Human Lactation, Vol. 31, No. 2, pp. 216–220, Jan. 2015, https://doi.org/10.1177/0890334414568315
-
E. Jaunet, A. Le Guern, P. Le Tacon, C. Thery-Dumeix, and M.-J. Deshayes, “Uncovering and treating asymmetry before 6years in our daily clinical practice: Option or obligation? Orthodontics or orthopedics?,” International Orthodontics, Vol. 11, No. 1, pp. 35–59, Mar. 2013, https://doi.org/10.1016/j.ortho.2012.12.013
-
B. Sargent, S. L. Kaplan, C. Coulter, and C. Baker, “Congenital muscular torticollis: bridging the gap between research and clinical practice,” Pediatrics, Vol. 144, No. 2, Aug. 2019, https://doi.org/10.1542/peds.2019-0582
-
W. Simões, Functional Jaw Orthopedics Through Neuro-Occlusal Rehabilitation. 2003.
-
A. Bashir, Fareeha Amjad, Ashfaq Ahmad, Ayesha Arooj, and Syed Amir Gilani, “Effect of physical therapy treatment in infants treated for congenital muscular torticollis – a narrative review,” Journal of the Pakistan Medical Association, Vol. 73, No. 1, pp. 111–116, Apr. 2022, https://doi.org/10.47391/jpma.3852
-
R. Fenton, S. Gaetani, Z. Macisaac, E. Ludwick, and L. Grunwaldt, “Description of mandibular improvements in a series of infants with congenital muscular torticollis and deformational plagiocephaly treated with physical therapy,” The Cleft Palate-Craniofacial Journal, Vol. 55, No. 9, pp. 1282–1288, Jul. 2018, https://doi.org/10.1177/1055665618763374
-
A. A. Kuo, S. Tritasavit, and J. M. Graham, “Congenital muscular torticollis and positional plagiocephaly,” Pediatrics in Review, Vol. 35, No. 2, pp. 79–87, Feb. 2014, https://doi.org/10.1542/pir.35-2-79
-
L. Stellwagen, E. Hubbard, and K. Vaux, “Look for the “stuck baby” to identify congenital torticollis,” Contemp Pediatr, Vol. 21, No. 5, pp. 55–65, 2004.
-
P. Planas, Neuro-Occlusal Rehabilitation and Flat Laws of Development of the Stomatognathic System. Rio de Janeiro: ED.Médica e Científica, 1997.
-
W. S. Simões, Functional Jaw Orthopedics. São Paulo: Artes Médicas, 2003.
About this article

I would like to thank my friend Dr. Valéria Medau for sharing all her knowledge and teachings.
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
The authors declare that they have no conflict of interest.
This study was approved by the institutional ethics committee under protocol number 6.808.201. All participants provided informed consent, and their confidentiality and anonymity will be preserved in accordance with applicable laws and regulations.
